News
Article
Breast Cancer Recurrence: High Adherence to Macro-Mediterranean Diet Hints Benefit
Author(s):
Macro-Mediterranean diets for patients with high-risk breast cancer recurrence found no overall reduction, but women who adhered more closely to the diet showed potential benefit.


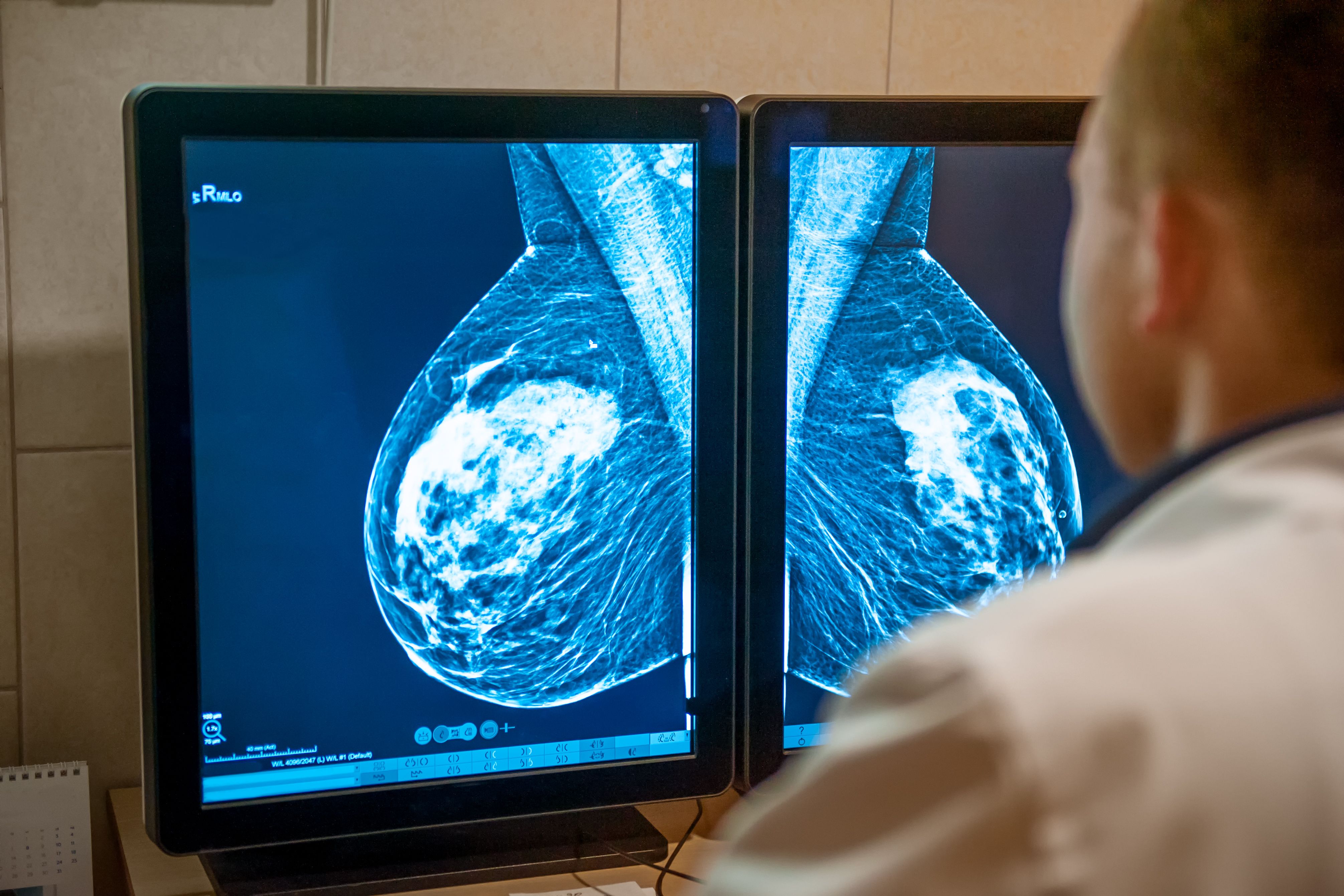
Breast Cancer, Macro-Mediterranean diet| Image Credit: r2 studio - stock.adobe.com

Breast cancer recurrence was not reduced by the DIet and ANdrogen (DIANA) randomized controlled trials but after 1 year, the intervention group (IG) and control group (CG) combined to display a protective association with the higher Dietary Index change.
The DIANA-5 trial investigated whether a specifically designed macro-Mediterranean diet could prevent breast cancer recurrence. This randomized controlled study targeted women with high-risk factors, including ER-negative tumors, metabolic syndrome, or elevated testosterone and insulin levels, that had undergone surgery over the last 5 years.
Several prior studies found better dietary habits are associated with improved survival among patients with breast cancer. Mediterranean diets consist of unrefined cereal products, pulses, vegetables, olive oil, nuts, fruits, moderate wine, and occasionally fish and cheese. It has shown improved body composition, insulin sensitivity, lipid profile, with associations to a lower cumulative incidence of metabolic syndrome.
There were 1,542 women recruited, aged 35 to 70 with a history of high-risk breast cancer but no current recurrence. These women, from 11 Italian institutions, were categorized into intervention (IG) and control (CG) groups, even if they were still undergoing hormonal therapy after completing chemotherapy.
The DIANA-5 intervention aimed to control weight and promote healthy eating. Dietary activities for the IG women consisted of thematic kitchen courses, community meals, they received menus, and recipes to support dietary changes. Participants were encouraged through “solidal buying groups” to utilize their use of organic and macrobiotic foods at home. Negotiations were made with organic food shops to obtain discounts for the participants too. Physical activity in IG women stressed the reduction of sedentary behavior and encouraged 30 minutes of moderate-intensity exercise daily. However, structured activity programs were limited due to low participation.
Breast cancer recurrence, the primary outcome of the DIANA-5 study, is displayed through the development of a new breast primary, ipsilateral or contralateral, local, or regional cancer recurrence, distant recurrence, or metastasis.
Of the total 1,542 women with high-risk recurrence of breast cancer, there were 769 randomized to the IG group and 773 into the CG group. Both groups had an 87% adherence of DIANA-5 activities and appointments in the first study year, but this reduced to 60% from the third to the fifth year.
Both groups improved after 1 year, but the IG women showed significantly greater changes. The IG women lost more weight (P < .001), had lower body mass indexes(P < .001), smaller waist circumferences (P < .001), improved blood sugar (P = .04) and triglycerides (P = .01). Additionally, the IG group saw a greater reduction in metabolic syndrome (P < .001) and a stronger shift towards recommended foods (2.8 vs 0.9; P < .001) while reducing consumption of discouraged foods (–3.4 vs –1.9; P < .001).
Despite a significant dietary change (average index difference, 3.1) in the intervention group, the DIANA-5 study found no overall reduction in breast cancer recurrence. Both groups had similar numbers of new events (95 vs 98) and distant metastases (55 vs 57). A subgroup analysis with higher compliance (498 participants) hinted at a potential benefit (lower HR), but results were inconclusive (HR, 0.58; 95% CI, 0.24-1.42).
A 41% reduction of new breast cancer events occurred in women with improvements above the upper tertile. Women classified above the upper tertile of change compared with women classified under the lower tertile, had an HR of 0.59. For the follow-up year, HRs were 0.98, 0.69, 0.52, 0.45, and 0.63.
On average, dietary index changes were an 11.1 upper tertile increase, 4.4 middle tertile increase, and a 1.8 lower tertile decrease. The average dietary index change above the upper tertile and below the lower tertile was 4 times greater than the IG and CG dietary index difference. Metabolic syndrome parameter improvements were not associated with better prognosis, except for blood pressure.
A limitation of the study was the failure to include precise tools to measure dietary intake, relying on a dietary index of unknown validity. While past research has not linked specific foods to breast cancer recurrence, further validation of the dietary index is necessary.
The study highlights the need for more intensive dietary interventions beyond monthly meetings and cooking classes to achieve a potential reduction in breast cancer recurrence, particularly for ER+ cases. While the macro-Mediterranean dietary goals did not show significant improvement in this study, future trials with more robust interventions are warranted.
Reference
Berrino F, Villarini A, Gargano G, et al. The effect of diet on breast cancer recurrence: The DIANA-5 randomized trial. Clin Cancer Res. 2024;30(5):965-974. doi:10.1158/1078-0432.CCR-23-1615