

|Articles|August 19, 2020
Supplements and Featured Publications
- Type 2 Diabetes: Current Data and Innovative Practices
Managing Type 2 Diabetes and the Role of Sodium-Glucose Cotransporter 2 Inhibitors
Advertisement
Impact of Type 2 Diabetes
Diabetes is a chronic, progressive disease. It is characterized by elevated blood glucose levels resulting from defects in the body related to insulin secretion, insulin action, or both.1-3 According to the 2020 CDC National Diabetes Statistics Report, an estimated 34.2 million Americans (about 1 in 10) have diabetes; type 2 diabetes (T2D) accounts for 90% to 95% of cases.4,5 Further, an additional 88 million American adults (1 in 3) have prediabetes, increasing their risk for T2D.6
T2D most often develops in people aged over 45 years, but children, teens, and young adults are also developing the disease in increasing numbers.4,5 Patients with diabetes often present with and are at a higher risk for comorbidities such as atherosclerotic cardiovascular disease (ASCVD), heart failure (HF), and renal disease.3,7-9 The results of a systematic review of global clinical records from a 10-year period showed that approximately one-third of patients with T2D had cardiovascular disease (CVD) as a comorbidity.10 Further, approximately two-thirds of deaths in people with diabetes are due to CVD, including ischemic heart disease, other forms of heart disease, principally congestive HF, and stroke.11
Additionally, the presence of HF is an independent risk factor for developing diabetes.9 About 12% of patients with T2D have established HF, and approximately 3.3% of patients with T2D develop HF each year.9 Further, the presence and severity of chronic kidney disease (CKD) highlights individuals with a heightened risk for adverse health outcomes, such as HF.12,13 The CDC estimates that approximately 1 in 3 Americans with diabetes may have CKD, with diabetes further accounting for 38% of reported causes of end-stage kidney disease in the United States.14 Further, in patients with diabetes, the presence of albuminuria is an independent risk factor for mortality.15
It is essential that health care providers identify predictors of excess mortality in patients with T2D to optimally target risk-reduction strategies. Patients with T2D would benefit from more aggressive preventive programs to prevent CVD. Programs that set stringent standards are more likely to reduce the incidence of cardiovascular morbidity and mortality.9
Treatment Goals and Guidelines
Treatment goals for T2D center on maintaining a patient’s quality of life by preventing or delaying associated complications and comorbidities. Treatment goals focus around glycemic control and CVD risk factor management. The American Diabetes Association (ADA) recommends regular patient follow-up and, importantly, a patient-centered approach to optimize treatment outcomes.16,17
Lifestyle modifications, including losing weight, increasing physical activity, and adopting a healthy diet, remain first-line strategies for the management of T2D.16,18 However, most patients with T2D are unable to control hyperglycemia with diet and exercise and require pharmacotherapy. Generally, monotherapy with an oral hypoglycemic agent is initiated; however, owing to the progressive nature of the disease, most patients will eventually require combination therapy and ultimately injectable treatments as monotherapy or part of polytherapy.19,20 The ADA states that early combination therapy can be considered in some patients at treatment initiation to extend the time to treatment failure.20 Pharmacologic therapy should take a stepwise approach, taking into account individual patient characteristics and the presence of comorbid diseases and complications.20
Prior consensus statements by the ADA and the European Association for the Study of Diabetes focus on efficacy in reducing hyperglycemia, with treatment tolerability and safety being primary factors in glucose-lowering medication selection.16,21 However, an update to treatment recommendations was added to the latest 2020 consensus report. This update is due to new evidence regarding the benefit of specific medications to reduce mortality, HF, and progression of renal disease in the setting of established CVD in patients with T2D.16,20
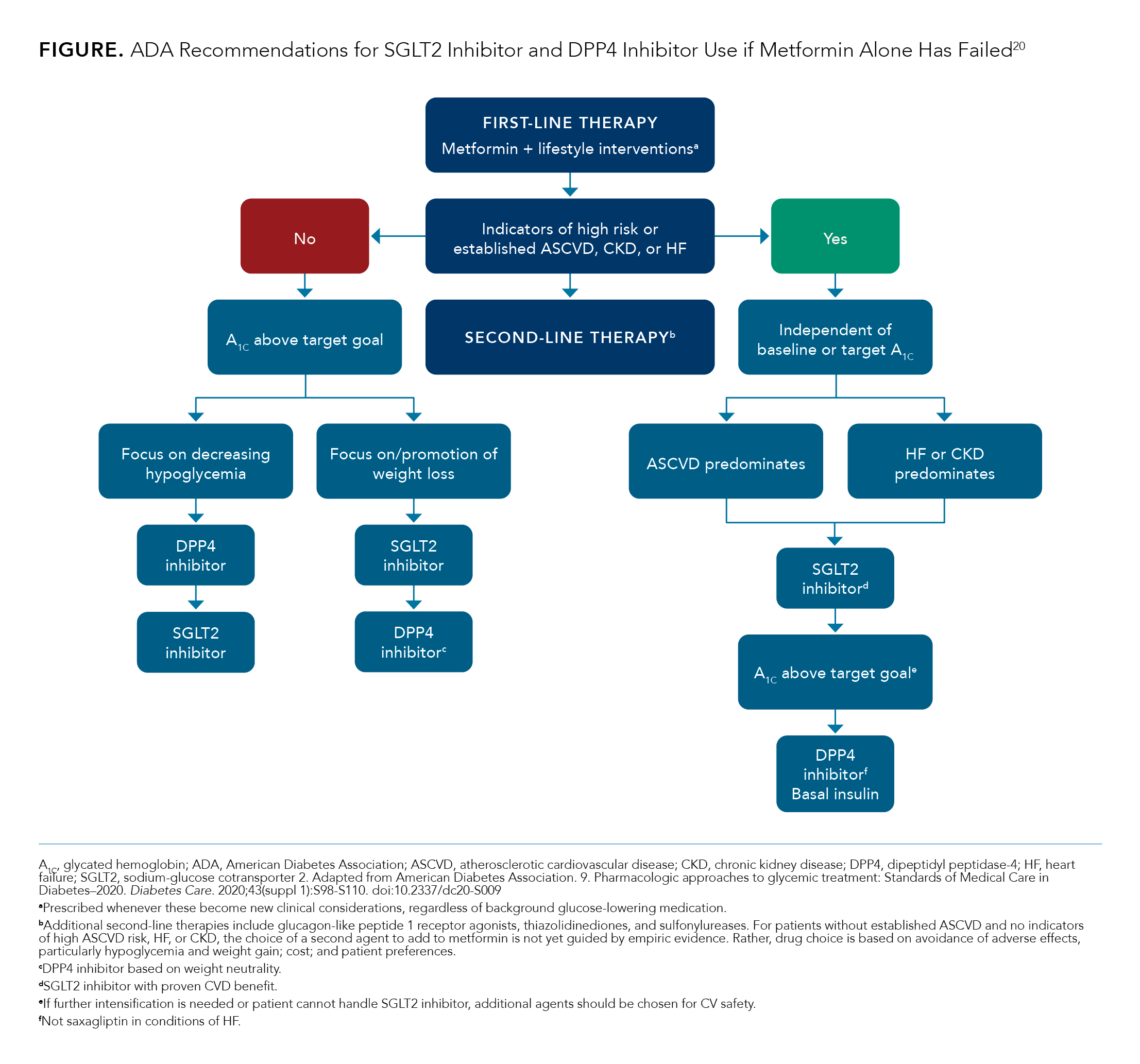
The ADA has adopted these updates in their 2020 recommendations, Standards of Medical Care: 9. Pharmacologic Approaches to Glycemic Treatment–2020 and 10. Cardiovascular Disease and Risk Management–2020.17,20 The current ADA T2D treatment guidelines are based on indicators of high risk or established ASCVD, CKD, and HF, with glycated hemoglobin (A1C) target levels also considered (
).20 The ADA has suggested a treatment cascade, initiating with monotherapy treatment (such as metformin) and progressing through dual or triple therapy options depending on patient characteristics and preferences (
).20
T2D Available Drug Treatment Options Per Updated ADA Guidelines
Metformin
The ADA states that metformin is the preferred initial pharmacologic agent for the treatment of T2D and should be started at the time T2D is diagnosed unless there are contraindications.20 However, as stated previously, T2D is a progressive disease and often requires additional therapy with combinations of drugs that have complementary mechanisms of action.22 As such, many patients will require dual combination therapy to achieve their target A1C level.20 Current recommendations are to use a stepwise addition of medications to metformin to maintain A1C at target levels (
).20
DPP4
Dipeptidyl peptidase-4 (DPP4) inhibitors are oral diabetic agents that are placed as an add-on second-line therapy after metformin failure as insulinotropic agents that have no intrinsic hypoglycemia risk.18,23 There are currently four DPP4 inhibitors available in the United States that have been approved by the FDA (
).24-40
All four DPP4 inhibitors appear to have similar efficacy in terms of glucose-lowering ability.40 A notable favorable characteristic of DPP4 inhibitors is their efficacy and safety profile in patients with impaired renal function.23 Further, in phase 3 clinical trials, DPP4 inhibitors have shown good safety and tolerability profiles. The most frequent adverse events (AEs) observed were nasopharyngitis and skin lesions, although 2 studies showed an increased rate of hospitalization due to HF.23,29,41,42 As CVD outcomes and safety are a concern for the T2D patient population, mortality and morbidity associated with therapy options should be considered when making treatment selections.
Several CVD outcomes trials have been completed, comparing DPP4 inhibitors with placebo against the backdrop of standard diabetes care, and the DPP4 inhibitors have been shown to have a neutral effect on CVD outcomes.40,41,43,44 Meta-analyses, however, suggest a possible increased risk of acute HF or hospitalized HF with certain DPP4 inhibitors versus placebo; more research is required to explore these observations.45,46 As DPP4 inhibitors come with the possible heightened risk of negative CVD effects, they are suggested as second-line therapy as an add-on to metformin in patients with T2D who need to control hypoglycemia but have no preexisting CVD.20,23,45
In assessing the cardiovascular safety profiles of antidiabetic drugs, sodium-glucose cotransporter 2 (SGLT2) inhibitor therapies have emerged with robust evidence for reducing the risk of adverse CVD outcomes in people with T2D who have either established CVD or are at risk of developing CVD and HF.8 Additional benefits have also been seen in those at risk of renal decline and progression to CKD.8
SGLT2 Inhibitors
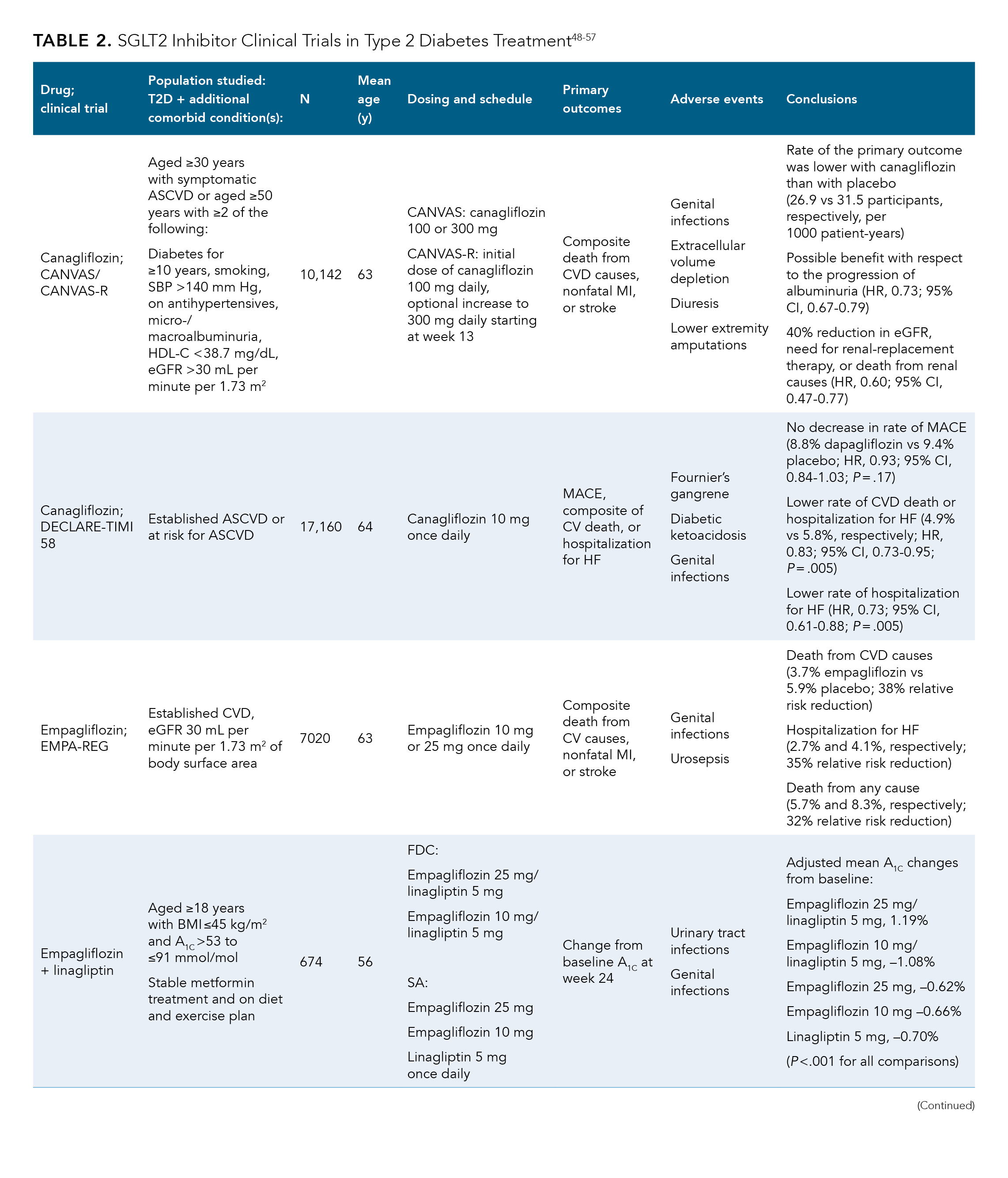
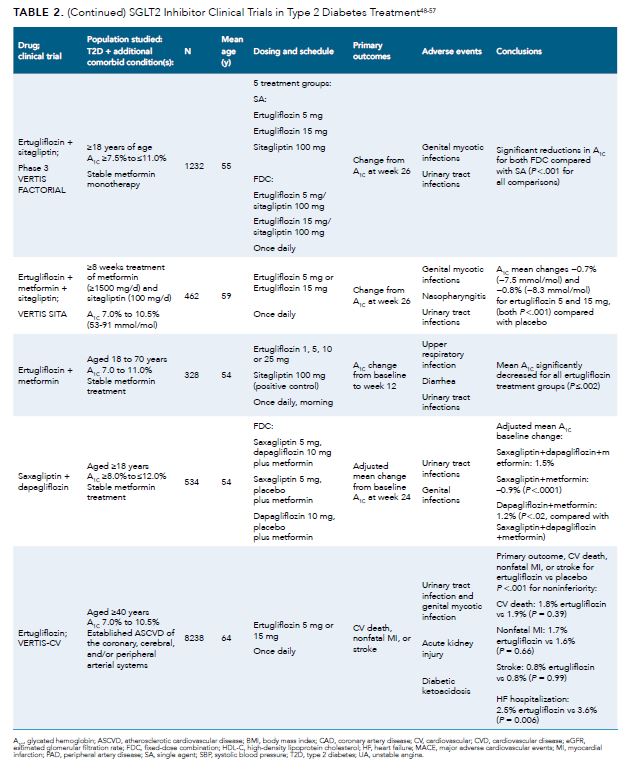
SGLT2 inhibitors are a fast-growing class of diabetes drugs given their convenient oral route of administration, strong A1C efficacy data, observed reductions in body weight, and antihypertensive effects. Importantly, these drugs show similar efficacy from early through late stages of diabetes.47 The FDA has approved four SGLT2 inhibitor–based therapies for use in T2D patients, as they have been shown to convey CVD protective effects and delay the progression of CKD;48-50 clinical trial data are summarized in
and
.48-57 The primary outcomes for all available studies were a combination of composite end points of CVD death, myocardial infarction (MI) or ischemic stroke, and HF or hospitalization due to HF.18,48-50 A reduction in risk of HF, MI, and stroke are the most common CVD benefits noted in SGLT2 inhibitor clinical studies (
and
).48-57 The most common AEs noted in most trials were an increased risk of genital infections in the SGLT2 inhibitor population compared with placebo, although the CANVAS trial also noted a higher incidence of amputations.48-50
Fixed-Dose Treatment Combinations
Although the above treatment options present favorable rationales for the use of each agent, there are current data to support initial combination therapy to more rapidly attain glycemic goals.58,59 Clinical trials have demonstrated that this approach is superior to sequential addition of medications, in terms of extending time to primary and secondary failure and decreasing risk of associated complications.60,61
DPP4 inhibitors and metformin-based fixed-dose combinations are accessible and may safely be used in T2D patients to reach treatment goals (
and
).23,48-57 Fixed-dose combinations of DPP4 and SGLT2 inhibitors can also be used (as dual therapy when metformin is contraindicated or not tolerated, or as triple therapy with metformin) to achieve treatment goals in patients with T2D (
and
).23,48-57 DPP4 and SGLT2 inhibitor combinations have complementary actions that have resulted in additive reductions of glycemic and blood pressure parameters.23,52 Findings of recent clinical trials of triple-therapy combinations with DPP4 and SGLT2 inhibitors have demonstrated significant clinical benefit over the use of each individual component when utilized on a background of metformin (
and
).48-57 A phase 3, randomized, double-blind, parallel-group study by Defronzo et al, examining different treatment combinations of empagliflozin and linagliptin as compared with each ingredient individually, noted more significant reductions in A1C levels from baseline for those patients receiving the combination treatments (P <.001 for all comparisons) (
and
).48-57 Further, SGLT2 inhibitors and metformin-based combinations have demonstrated reductions in glycemia, blood pressure, body weight, and albuminuria in people with diabetes.48,53-55,62 A study by Pratley et al demonstrated that in T2D patients with inadequate glycemic control with metformin, co-administration of ertugliflozin (5 or 15 mg) with sitagliptin (100 mg) provided significantly greater improvements in measures of glycemic control compared with addition of either agent alone (P <.001 for all comparisons).53 Notably, in a phase 3 randomized double-blind, active controlled, parallel group study, patients on a fixed dose treatment of saxagliptin + dapagliflozin + metformin experienced a lower rate of AE compared with those patients on treatments of either saxagliptin or dapagliflozin alone.56
While these results illustrate that a fixed-dose combination treatment can help attain T2D treatment goals, the choice of treatment should be tailored to each individual and their T2D prognosis and comorbidities. For those patients with T2D and no elevated CV risk DPP4 inhibitors, such as sitagliptin, are a safe and effective treatment option and can lead to similar treatment outcomes. A randomized, double-blind, placebo- and active-controlled, parallel group, double-dummy, dose-ranging study by Amin et al demonstrated that a lower dose combination of ertugliflozin (5 mg) plus metformin lead to similar A1C reductions when compared with a higher dose of sitagliptin (100 mg) alone.55 Ultimately a the choice of treatment regimen should be made through an open dialogue taking into consideration patient treatment goals, T2D comorbidities, and patient lifestyle and preferences.
Summary
Despite more than 200 years of research on lifestyle management of diabetes and more than 50 years of comparative-effectiveness research in diabetes, innumerable unanswered questions regarding the management of T2D remain.16 T2D treatment guidelines have evolved to adapt to the larger picture of disease, but T2D still carries a significant burden of illness and unmet need. T2D treatment is further complicated by patient comorbidities and their associated risk factors. Optimizing treatment pathways can help alleviate the burden of disease and reach treatment goals for this patient population.
SGLT2 inhibitors, a new option recommended by the ADA 2020 guidelines either as single agents or in fixed-dose combinations with other treatments, offer patients the option to take advantage of benefits beyond stabilization of A1C levels. SGLT2 inhibitors have shown favorable CVD effects, including a reduction in the risk of hospitalization for HF, predominantly in patients with T2D and established CVD48,49,51; they have also been shown to delay the progression of kidney disease.51
References
- Deshpande AD, Harris-Hayes M, Schootman M. Epidemiology of diabetes and diabetes-related complications. Phys Ther. 2008;88(11):1254‐1264. doi:10.2522/ptj.20080020
- American Diabetes Association. Standards of medical care in diabetes–2006. Diabetes Care. 2006;29(Suppl 1):S4‐S42. Published correction appears in Diabetes Care. 2006;29(5):1192. doi:10.2337/dc06-0805
- IDF Atlas, 9th edition–2019. International Diabetes Federation. Accessed May 10, 2020. https://www.diabetesatlas.org/en/
- National Diabetes Statistics Report. CDC. Updated February 14, 2020. Accessed May 7, 2020. https://www.cdc.gov/diabetes/data/statistics/statistics-report.html
- CDC,2019 Type 2 diabetes. CDC. Updated May 30, 2019. Accessed May 2, 2020. https://www.cdc.gov/diabetes/basics/type2.html
- CDCPrediabetes,2020 Prediabetes – your chance to prevent type 2 diabetes. CDC. Updated June 11, 2020. Accessed June 19, 2020. https://www.cdc.gov/diabetes/basics/prediabetes.html
- American Diabetes Association. 4. Comprehensive medical evaluation and assessment of comorbidities: Standards of Medical Care in Diabetes–2020. Diabetes Care. 2020;43(Suppl 1):S37‐S47. doi:10.2337/dc20-S004
- Ali A, Bain S, Hicks D, et al; the Improving Diabetes Steering Committee. SGLT2 inhibitors: cardiovascular benefits beyond HbA1c—translating evidence into practice. Diabetes Ther. 2019;10(5):1595‐1622. doi:10.1007/s13300-019-0657-8. Published correction appears in Diabetes Ther. 2019;10(5):1623-1624. doi:10.1007/s13300-019-0670-y.
- Bell DSH. Heart failure: the frequent, forgotten, and often fatal complication of diabetes. Diabetes Care. 2003;26(8):2433‐2441. doi:10.2337/diacare.26.8.2433
- Einarson TR, Acs A, Ludwig C, Panton UH. Prevalence of cardiovascular disease in type 2 diabetes: a systematic literature review of scientific evidence from across the world in 2007-2017. Cardiovasc Diabetol. 2018;17(1):83. doi:10.1186/s12933-018-0728-6
- Low Wang CC, Hess CN, Hiatt WR, Goldfine AB. Clinical update: cardiovascular disease in diabetes mellitus: atherosclerotic cardiovascular disease and heart failure in type 2 diabetes mellitus – mechanisms, management, and clinical considerations. Circulation. 2016;133(24):2459‐2502. doi:10.1161/CIRCULATIONAHA.116.022194
- Thomas MC. Type 2 diabetes and heart failure: challenges and solutions. Curr Cardiol Rev. 2016;12(3):249‐255. doi:10.2174/1573403x12666160606120254
- De Cosmo S, Viazzi F, Pacilli A, et al; AMD-Annals Study Group. Predictors of chronic kidney disease in type 2 diabetes: a longitudinal study from the AMD Annals initiative. Medicine (Baltimore). 2016;95(27):e4007. doi:10.1097/MD.0000000000004007. Published correction appears in Medicine (Baltimore). 2016;95(49):e5660. doi:10.1097/MD.0000000000005660
- CDCKD,2019 Chronic kidney disease in the United States, 2019. CDC. Updated March 11, 2019. Accessed May 7, 2020. https://www.cdc.gov/kidneydisease/publications-resources/2019-national-facts.html#:~:text=CKD%20Is%20Common%20Among%20US%20Adults&text=CKD%20is%20more%20common%20in,%2DHispanic%20Asians%20(12%25)
- Bermejo S, González E, López-Revuelta K, et al. Risk factors for non-diabetic renal disease in diabetic patients. Clin Kidney J. 2020:1-9. doi: 10.1093/ckj/sfz177
- Davies MJ, D’Alessio DA, Fradkin J, et al. Management of hyperglycaemia in type 2 diabetes, 2018. a consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetologia. 2018;61(12):2461-2498. doi:10.1007/s00125-018-4729-5. Correction appears in Diabetologia. 2019;62(5):873.
- American Diabetes Association. 10. Cardiovascular disease and risk management: Standards of Medical Care in Diabetes–2019. Diabetes Care. 2019;42(Suppl 1):S103‐S123. doi:10.2337/dc19-S010
- Garber AJ, Abrahamson MJ, Barzilay JI, et al. Consensus statement by the American Association of Clinical Endocrinologists and American College of Endocrinology on the comprehensive type 2 diabetes management algorithm – 2017 executive summary. Endocr Pract. 2017;23(2):207‐238. doi:10.4158/EP161682.CS
- García-Pérez LE, Alvarez M, Dilla T, et al. Adherence to therapies in patients with type 2 diabetes. Diabetes Ther. 2013;4(2):175‐194. doi:10.1007/s13300-013-0034-y
- American Diabetes Association. 9. Pharmacologic approaches to glycemic treatment: Standards of Medical Care in Diabetes–2020. Diabetes Care. 2020;43(Suppl 1):S98-S110. doi:10.2337/dc20-S009
- Buse JB, Wexler DJ, Tsapas A, et al. Diabetes Care. 2020;43:487–493. doi:10.2337/dci19-0066
- Inzucchi SE, Bergenstal RM, Buse JB, et al. Management of hyperglycemia in type 2 diabetes, 2015: a patient-centered approach: update to a position statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care. 2015;38(1):140‐149. doi:10.2337/dc14-2441
- Gallwitz B. Clinical use of DPP-4 inhibitors. Front Endocrinol (Lausanne). 2019;10:389. doi:10.3389/fendo.2019.00389
- Inovamet. Prescribing information. Janssen Pharmaceuticals; 2020. Accessed May 12, 2020. http://www.janssenlabels.com/package-insert/product-monograph/prescribing-information/INVOKAMET+XR-pi.pdf
- Linagliptin. Prescribing information. Boehringer Ingelheim Pharmaceuticals; 2020. Accessed May 10, 2020. https://docs.boehringer-ingelheim.com/Prescribing%20Information/PIs/Tradjenta/Tradjenta.pdf
- Jentadueto. Prescribing information. Boehringer Ingelheim Pharmaceuticals; 2020. Accessed May 10, 2020. https://docs.boehringer-ingelheim.com/Prescribing%20Information/PIs/Jentadueto/Jentadueto.pdf
- Farxiga. Prescribing information. AstraZeneca; 2020. Accessed May 10, 2020. https://www.azpicentral.com/farxiga/farxiga.pdf
- Xiyduo. Prescribing information. AstraZeneca; 2020. Accessed May 15, 2020. https://www.azpicentral.com/xigduoxr/xigduoxr.pdf
- Saxagliptin. Prescribing information. AstraZeneca; 2020. Accessed May 15, 2020. https://www.accessdata.fda.gov/drugsatfda,docs/label/2009/022350lbl.pdf
- Kombiglyze. Prescribing information. AstraZeneca; 2019. https://www.azpicentral.com/kombiglyzexr/kombiglyzexr.pdf
- Qtem. Prescribing information. AstraZeneca; 2020. Accessed May 15, 2020. https://www.azpicentral.com/qtern/qtern.pdf
- Jardiance. Prescribing information. Boehringer Ingelheim Pharmaceuticals; 2020. Accessed May 15, 2020. https://docs.boehringer-ingelheim.com/Prescribing%20Information/PIs/Jardiance/jardiance.pdf
- Synardy. Prescribing information. Boehringer Ingelheim Pharmaceuticals; 2020. Accessed May 10, 2020. https://docs.boehringer-
- Januvia. Prescribing information. Merck & Co; 2020. Accessed May 15, 2020. https://www.merck.com/product/usa/pi,circulars/j/januvia/januvia,pi.pdf
- Janumet. Prescribing information. Merck & Co; 2020. Accessed May 15, 2020. https://www.merck.com/product/usa/pi,circulars/j/janumet/janumet,pi.pdf
- Glyxambi. Prescribing information. Boehringer Ingelheim Pharmaceuticals; 2020. Accessed May 10, 2020. https://docs.boehringer-ingelheim.com/Prescribing%20Information/PIs/Glyxambi/Glyxambi.pdf
- Steglatro. Prescribing information. Merck & Co; 2020. Accessed May 15, 2020. ingelheim.com/Prescribing%20Information/PIs/Synjardy/Synjardy.pdf
- Segluromet. Prescribing information. Merck & Co; 2020. Accessed May 15, 2020. https://www.merck.com/product/usa/pi,circulars/s/segluromet/segluromet,pi.pdf
- Steglujan. Prescribing information. Merck & Co; 2020. Accessed May 15, 2020. https://www.merck.com/product/usa/pi,circulars/s/steglujan/steglujan,pi.pdf
- Wilding JPH, Panicker Rajeev S, DeFronzo RA. Positioning SGLT2 inhibitors/incretin-based therapies in the treatment algorithm. Diabetes Care. 2016;39(Suppl 2):S154‐S164. doi:10.2337/dcS15-3005
- Scirica BM, Bhatt DL, Braunwald E, et al. Saxagliptin and cardiovascular outcomes in patients with type 2 diabetes mellitus. N Engl J Med. 2013;369(14):1317-1326. doi:10.1056/NEJMoa1307684
- Zannad F, Cannon CP, Cushman WC, et al. Heart failure and mortality outcomes in patients with type 2 diabetes taking alogliptin versus placebo in EXAMINE: a multicentre, randomised, double-blind trial. Lancet. 2015;385(9982):2067-2076. doi:10.1016/S0140-6736(14)62225-X
- Green JB, Angelyn Bethel M, Armstrong PW, et al; TECOS Study Group. Effect of sitagliptin on cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2015;373(3):232‐242. doi:10.1056/NEJMoa1501352. Published correction appears in N Engl J Med. 2015;373(6):586. doi:10.1056/NEJMx1500029
- Rosenstock J, Kahn SE, Johansen OE, et al. Effect of linagliptin vs glimepiride on major adverse cardiovascular outcomes in patients with type 2 diabetes: The CAROLINA randomized clinical trial. JAMA. 2019;322(12):1155-1166. doi:10.1001/jama.2019.13772. Correction appears in JAMA. 2019;322(21):2138.
- Clifton P. Do dipeptidyl peptidase IV (DPP-IV) inhibitors cause heart failure?. Clin Ther. 2014;36(12):2072‐2079. doi:10.1016/j.clinthera.2014.10.009
- Monami M, Dicembrini I, Mannucci E. Dipeptidyl peptidase-4 inhibitors and heart failure: a meta-analysis of randomized clinical trials. Nutr Metab Cardiovasc Dis. 2014;24(7):689‐697. doi:10.1016/j.numecd.2014.01.017
- Zhang L, Feng Y, List J, et al. Dapagliflozin treatment in patients with different stages of type 2 diabetes mellitus: effects on glycaemic control and body weight. Diabetes Obes Metab. 2010;12(6):510‐516. doi:10.1111/j.1463-1326.2010.01216.x
- Neal B, Perkovic V, Matthews DR. Canagliflozin and cardiovascular and renal events in type 2 diabetes. N Engl J Med. 2017;377(21):2099. doi:10.1056/NEJMc1712572
- Zinman B, Wanner C, Lachin JM, et al; EMPA-REG OUTCOME Investigators. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med. 2015;373(22):2117‐2128. doi:10.1056/NEJMoa1504720
- Wiviott SD, Raz I, Bonaca MP, et al; DECLARE-TIMI 58 Investigators. Dapagliflozin and cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2019;380(4):347‐357. doi:10.1056/NEJMoa1812389
- Mahaffey KW, Neal B, Perkovic V, et al; CANVAS Program Collaborative Group. Canagliflozin for primary and secondary prevention of cardiovascular events: results from the CANVAS program (Canagliflozin Cardiovascular Assessment Study). Circulation. 2018;137(4):323‐334. doi:10.1161/CIRCULATIONAHA.117.032038
- DeFronzo RA, Lewin A, Patel S, et al. Combination of empagliflozin and linagliptin as second-line therapy in subjects with type 2 diabetes inadequately controlled on metformin. Diabetes Care. 2015;38(3):384‐393. doi:10.2337/dc14-2364. Published correction appears in Diabetes Care. 2015;38(6):1173. doi:10.2337/dc15-er06
- Pratley RE, Eldor R, Raji A, et al. Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with type 2 diabetes mellitus inadequately controlled with metformin: the VERTIS FACTORIAL randomized trial. Diabetes Obes Metab. 2018;20(5):1111‐1120. doi:10.1111/dom.13194
- Dagogo-Jack S, Liu J, Eldor R, et al. Efficacy and safety of the addition of ertugliflozin in patients with type 2 diabetes mellitus inadequately controlled with metformin and sitagliptin: the VERTIS SITA2 placebo-controlled randomized study. Diabetes Obes Metab. 2018;20(3):530‐540. doi:10.1111/dom.13116
- Amin NB, Wang X, Jain SM, et al. Dose-ranging efficacy and safety study of ertugliflozin, a sodium-glucose co-transporter 2 inhibitor, in patients with type 2 diabetes on a background of metformin. Diabetes Obes Metab. 2015;17(6):591‐598. doi:10.1111/dom.12460
- Rosenstock J, Hansen L, Zee P, et al. Dual add-on therapy in type 2 diabetes poorly controlled with metformin monotherapy: a randomized double-blind trial of saxagliptin plus dapagliflozin addition versus single addition of saxagliptin or dapagliflozin to metformin. Diabetes Care. 2015;38(3):376-383. doi:10.2337/dc14-1142
- Cannon CP, McGuire DK, Cherney D, et al. Results of the eValuation of ERTugliflozin EffIcacy and Safety CardioVascular Outcomes Trial (VERTIS CV). Presented at: 80th American Diabetes Association Scientific Sessions; June 16, 2020. Symposium.
- Milder TY, Stocker SL, Abdel Shaheed C, et al. Combination therapy with an SGLT2 inhibitor as initial treatment for type 2 diabetes: a systematic review and meta-analysis. J Clin Med. 2019;8(1):45. doi:10.3390/jcm8010045
- Phung OJ, Sobieraj DM, Engel SS, Rajpathak SN. Early combination therapy for the treatment of type 2 diabetes mellitus: systematic review and meta-analysis. Diabetes Obes Metab. 2014;16(5):410‐417. doi:10.1111/dom.12233
- Laiteerapong N, Ham SA, Gao Y, et al. The legacy effect in type 2 diabetes: impact of early glycemic control on future complications (the Diabetes & Aging study). Diabetes Care. 2019;42(3):416‐426. doi:10.2337/dc17-1144
- Matthews DR, Paldánius PM, Proot P, et al; VERIFY Study Group. Glycaemic durability of an early combination therapy with vildagliptin and metformin versus sequential metformin monotherapy in newly diagnosed type 2 diabetes (VERIFY): a 5-year, multicentre, randomised, double-blind trial. Lancet. 2019;394(10208):1519‐1529. doi:10.1016/S0140-6736(19)32131-2
- Rosenstock J, Frias J, Páll D, et al. Effect of ertugliflozin on glucose control, body weight, blood pressure and bone density in type 2 diabetes mellitus inadequately controlled on metformin monotherapy (VERTIS MET) Diabetes Obes Metab. 2018;20(3):520‐529. doi:10.1111/dom.13103. Published correction appears in Diabetes Obes Metab. 2018;20(11):2708. doi:10.1111/dom.13533
Articles in this issue
Advertisement
Related Content




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Advertisement
Advertisement
Trending on AJMC
1
FDA Approves First Oral Carbapenem Antibiotic for Complicated UTIs
2
5 Ongoing Clinical Trials in Myeloproliferative Neoplasms
3
Fourteen Years of HIV PrEP: How New Innovations Build on Decades of Progress in HIV
4
Walcker Named President of Cardinal’s The Specialty Alliance, With Strengths in GI, Urology
5