

|Articles|August 19, 2020
Supplements and Featured Publications
- Type 2 Diabetes: Current Data and Innovative Practices
Optimizing Outcomes From Pharmacologic Management of Type 2 Diabetes
Advertisement
Impact of Type 2 Diabetes on Patient Outcomes and the Health Care System
The burden of type 2 diabetes (T2D) is considerable and extends to those individuals living with comorbid conditions and the health care systems that support them. In 2017, the total cost incurred by those with diagnosed diabetes in the United States was $327 billion compared with $245 billion in 2012, when the cost was last examined.1,2 After accounting for inflation, this represents a 26% increase during the 5-year period evaluated, due in part to the increasing prevalence of diabetes.1,2 The American Diabetes Association (ADA) noted that the largest drivers of the cost of diabetes are higher use of prescription medications beyond antihyperglycemic medications; higher use of inpatient services, medications, and supplies to directly treat T2D; and more office visits to physicians and other health providers, compared with patients without T2D.1
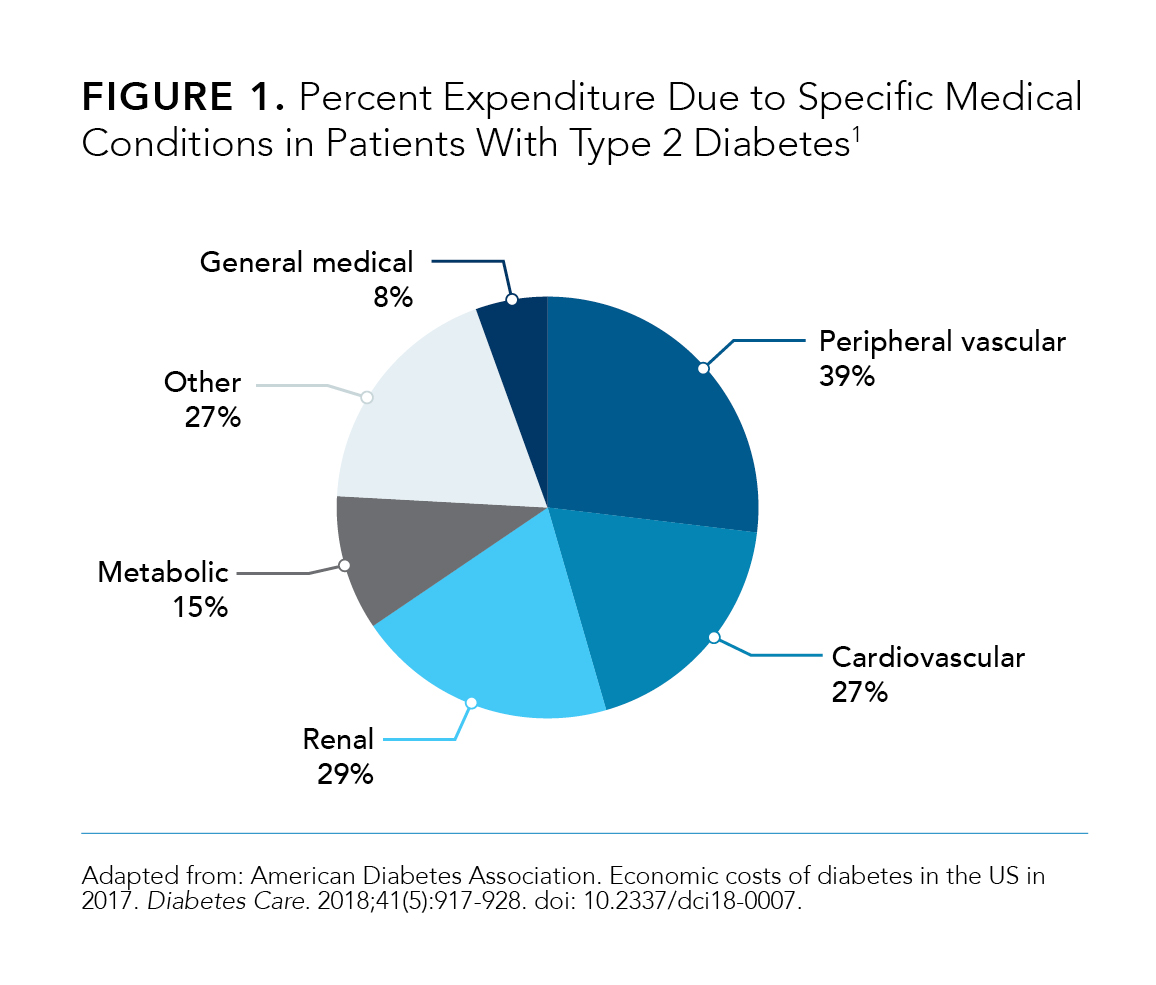
Adding to the complexities of diabetes cost and treatment are associated risk factors, as well as comorbidities such as cardiovascular disease (CVD) (
1).3 In 2017, the ADA estimated that $37.3 billion was spent in cardiovascular-related costs incurred by patients with diabetes.1 The results of a 2015 retrospective, cross-sectional study of the claims of 1,202,596 patients from the MarketScan database showed that the total health care costs of patients with T2D and concomitant atherosclerotic cardiovascular disease (ASCVD) were more than doubled compared with those of patients with T2D alone. Of that, medical (outpatient, inpatient, and emergency department visits) costs were 3 times higher and pharmacy costs were approximately 40% higher among patients with T2D and ASCVD comparedwith patients with T2D but not ASCVD.3
Further, the presence of at least 1 additional comorbidity, such as CVD, not only adds to the complexity and cost of treating T2D but is also associated with increased health care service utilization.3,4 The results of a 2006 retrospective health care registration study by Struijs et al demonstrated health care utilization among patients with T2D increased in tandem with the number of comorbidities.4 It was noted that patients with only T2D had fewer health care specialist consultations, overall hospital admissions, and hospital stay days compared with those individuals with T2D and any vascular or nonvascular–related comorbidity.4 Similar results were shown by Weng et al in a 2020 retrospective, cross-sectional study of 2015 US claims data, the results of which demonstrated that patients with T2D and ASCVD had visited physicians more frequently and had a higher number of annual visits compared with patients with T2D only.3 The results of this study also demonstrated a 3.5-fold number of hospital inpatient visits in those patients with T2D and ASCVD (15.6%) compared those with T2D only (4.4%).3
Further, the results of a 2013 cluster randomized controlled trial by Teljeur et al highlighted an association between the number of chronic conditions a patient has and polypharmacy.5 This study illustrated a nearly 2-fold increase in polypharmacy in patients with more than 1 chronic condition compared with patients with only 1.5 Multimorbidity can have implications in an individual’s disease management, and awareness of this association could lead to better treatment outcomes.5
Lastly, the prevalence of diabetes has increased at a more pronounced rate among certain populations, including racial/ethnic minorities and individuals with a lower level of education.6 The results of a 2011 prospective, randomized, placebo-controlled study by Lee et al noted an inverse relationship between diabetes incidence and both level of education and income.7 Additionally, the results of a 2009 community-based epidemiologic survey completed by Link et al demonstrated that the more important indicator when determining rates of diabetes is socioeconomic status (SES), compared with race or ethnicity.8
A better understanding of the relationship of these comorbid and SES associations will improve the development of cost-effective, culturally tailored programs for patients with T2D that are sensitive to the needs of the populations being served. It is particularly important to identify areas that providers and health care organizations might focus on to simultaneously lower costs and improve care.
Challenges Facing Patients With T2D Leading to Poor Management and Nonadherence
In the United States, societal costs compounded with increasing diabetes prevalence, morbidity, and mortality create immense health care challenges.9 The ADA recognizes the association between social and environmental factors and diabetes and the necessity of considering these factors when working to prevent, manage, and treat diabetes.10 Novel strategies are required to address these social and environmental factors when providing care to patients with T2D (
).11
One area of promise involves improving care coordination. Models that incorporate novel education techniques and drug combinations have demonstrated success in improving glycated hemoglobin (A1C) control, reducing excess health care utilization, and increasing patients’ treatment adherence and access to care.9,12-15
Education
“Diabetes self-management education/training (DSME) is the ongoing process of facilitating the knowledge, skill, and ability necessary for diabetes self-care.”16 It has been shown that the first 6 months to 4 years after diagnosis are crucial to the long-term management of T2D.17 The specific goals of DSME are as follows: explaining the basic concepts of T2D; illustrating the importance of identifying and counting carbohydrates; describing the benefits of maintaining a healthy body weight and exercising regularly; and monitoring and controlling blood sugar via medication planning, management, and administration.17-20
Despite its proven benefits, the number of individuals with T2D who receive DSME is low.21 Low rates of DSME uptake and utilization are influenced by patient-specific and health system-specific barriers that can affect the attainment of optimal health status (
).11 Patient-specific barriers can include financial and logistical access to DSME, such as difficulty accessing transportation to care sessions, which may affect populations that live within rural communities and those without health care coverage.19
New platforms such as electronic delivery (computer and telephone) and the use of community-based group educational settings offer potential for greater patient access and uptake of DSME.9,11,14,19 The results of a 2018 cluster randomized trial by Sood et al demonstrated that the use of electronic telecommunication decreased a patient’s need for travel and provided an effective means of communication between the patient and their entire care team.11
Cost and Health Care Economics
As mentioned previously, the high cost of managing diabetes presents a growing challenge for health care systems and patients. Out-of-pocket (OOP) costs and health care system utilization costs (eg, those related to inpatient, outpatient, and emergency department visits) can influence the therapies that physicians suggest and patients ultimately use.22,23
The cost of medication can be a major deterrent toward achieving treatment goals and patient adherence.1,10 As such, less costly treatment options which lead to greater health outcomes should be considered in line with drug safety and efficacy, associated comorbidities, and patient lifestyles and preferences. New drug classes of treatments (eg, SGLT2 and DPP4 inhibitors) present an opportunity to overcome these challenges due to the potential to reduce health care costs outside of the medication cost alone. SGLT2 and DPP4 inhibitors and fixed-dose combinations demonstrate reductions in hospitalizations and heightened health benefits relating to weight reduction, A1C levels, and CVD risk.24
A 2018 retrospective observational study examining de-identified patient data from 4 observational databases compared the risk of hospitalization due to heart failure (HHF) between new SGLT2 inhibitors and other anti-hyperglycemic agents (AHA) users.25 The use of SGLT2 inhibitors versus other available AHAs lead to an overall lower risk of HHF for patients with T2D (95% CI, 0.39 [0.26-0.60]) and reached significance for those patients with established CVD.25 These health care utilization reductions were demonstrated to lead to a significant decrease in all-cause health care costs (P <.0001).26
DPP4 inhibitors, listed as a second line treatment by the ADA, may be a cost-effective treatment option for those patients with low CVD risk and who attain their A1C and weight loss goals.27 DPP4 inhibitors are weight neutral, show benefits in hypoglycemia, and carry low adverse reactions.27 If treatment goals remain uncontrolled on DPP4 inhibitors, the escalation or addition of alternate therapies (eg, SGLT2 inhibitors or fixed-dose combinations) can further mitigate cost and enhance patient health outcomes by decreasing prescription costs and greater attainment of treatment goals.
In 2018, the ADA estimated the total costs of the treatment of diagnosed diabetes in the United States. The majority (67%) of these costs are covered by government-provided insurance (ie, Medicare, Medicaid, and military). Private insurance (31%) and the uninsured (2%) make up the rest of the costs.2
Research has revealed substantial disparities in health and access to health care services across SES groups in the United States.7,28-30
A 2007 cross-sectional study by Nwasuruba et al utilized data collected via a telephone-based survey and demonstrated racial differences in self-care behaviors in patients with T2D. Self-care behaviors, such as attaining the recommended number of physical activity minutes or engaging in at home self-monitoring of blood glucose, were diminished in black and Hispanic populations compared with white populations.29
Health care insurance type and access were also demonstrated to affect A1C levels based on the results of a 2019 cross-sectional study in which Liese et al evaluated surveillance data from 481 youth and young adults with a diagnosis of diabetes. The results illustrated a protective effect of private insurance on A1C levels when compared with individuals with state or federal insurance (P = .0025) or no insurance (P <.0001).31
Further, the results of 2017 cross-sectional study by Assari et al demonstrated that SES and governmental insurance may be predictors of A1C control and may be influenced by characteristics such as age, race, and gender, although the study lacks generalizability due to sample size.30 For example, for black men, age (P = .040) and having governmental insurance (P = .042), were correlated with A1C.30 In another study of SES in relation to diabetes care, Arpey et al (2017) conducted patient interviews to evaluate patients’ perceptions to care in relation to their SES status. They noted that most subjects felt their SES status influenced the type and amount of care they received. Individuals also felt that their SES altered the amount, type, and ability to schedule needed tests and obtain medications.32
SES is a potentially modifiable risk factor for disease that should be targeted for early implementation of public health strategies aimed at improving SES disparities for vulnerable populations.7 Public health policies and guidelines created with community based initiatives can ensure clinical benefits are achieved across SES groups.
Effective partnerships among medical care, social services, public health, and community-based organizations could improve population health outcomes by addressing the social determinants of health. A retrospective evaluation of a 12‐month pilot diabetes care program in a rural setting by McLendon et al noted that DSME was successful due to strong partnerships with a community advisory network, health care leadership representatives, and 2 primary care host sites within the rural community, allowing for the successful execution of their pilot care model program.9 Quinoñes et al (2015) noted that community health workers can bolster and build personal connections between health care systems and patients to ease the difficulty of navigating these complex systems. These workers can increase access to care by illuminating pathways to limited community resources, helping patients understand their care options, and helping to tailor treatment interventions to encompass social and cultural needs.28
Various interventions, such as reducing patient cost sharing, have been suggested to decrease SES disparities in health care, and studies looking at cost sharing in patients with T2D have demonstrated an inverse relationship between cost and attainment of treatment goals and medication adherence.33,34 Henk et al noted that for patients enrolled in fixed tiered plans, a 10% higher medication copayment led to a significant reduction (P <.001) in medication adherence.33
A 2016 retrospective cohort study of medical and pharmacy claims data from 2004 to 2012 from 92,410 patients with T2D enrolled in 1514 health care plans evaluated the associations among cost sharing, medication adherence, and per-patient all-cause hospital days. Results of this study showed a 1.6% point decrease in adherence (2.4%; P <.01) with a $10 increase in patient OOP cost. A 10% reduction in adherence was associated with 15% more per-patient hospital days.34
Comprehensive care models should account for costs, value, and clinical outcomes to the patient to be the most cost and clinically beneficial.34 Given that health care-related costs in the United States have continued to rise, many stakeholders are looking to novel means to optimize the value of health care. Programs focusing on incentivizing optimal clinical outcomes for patients are being explored (eg, consumer-driven health plans, wellness and prevention programs, pay-for-performance initiatives, and health information technology tracking). Programs may prove most successful to the patient and health care ecosystem when they are able to both benefit health-related behaviors and mitigate costs.35
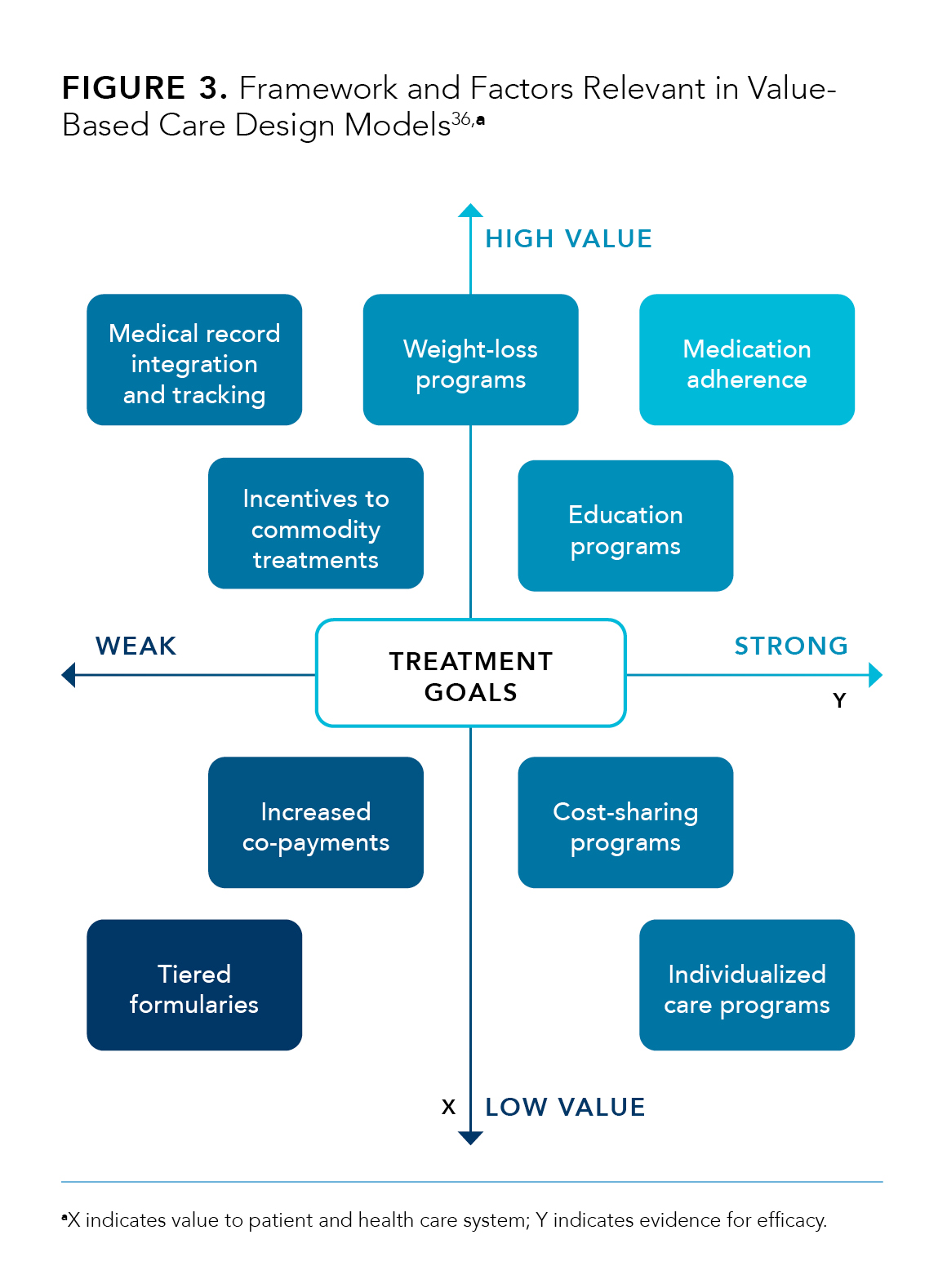
Strategies to move toward value-based care, a system that provides incentives for the attainment of treatment goals, may prove helpful to reducing cost and treatment burden. Value-based packages are created to motivate positive clinical outcomes by providing financial incentives to patients and clinicians to use certain treatments by employing lower OOP costs and higher reimbursement, respectively (
).36 In patients with T2D, these value-based systems need to go beyond A1C levels and encompass comorbidities like CVD and heart failure. The ADA has included treatment agents with protective effects against CVD (eg, sodium-glucose cotransporter 2 inhibitors) into their guidelines in tandem with other first-line agents for patients with comorbid CVD and T2D, based on their potential to decrease cardiovascular events.27 Value-based partnerships that capitalize on these ADA recommendations have the potential to decrease the cost of T2D care and improve patient outcomes.
Access to T2D Care
Care coordination by both patient and their health care provider are required to elicit optimal care.37 In order to be inclusive patient centered care programs cannot assume a standardized level of access to care.37 According to Nash et al, 3 unique steps are key to obtain appropriate access to care: “gaining entry into the health care system; (2) getting access to care settings where the patient can receive needed services; and (3) finding providers who meet the needs of individual patients and with whom patients can develop a relationship based on mutual communication and trust.”37
Access to treatment can further be compounded by a lack of knowledge or understanding of treatment option by both patient and provider.37 The establishment of T2D treatment guidelines and care centers through public or private policy should be accessible to patients regardless of income, self-care ability, or living situation.37
One crucial potential barrier to accessing T2D treatment is a patient’s geographic location. For instance, in rural areas, distance to treatment centers, inclement weather, a lack of public transportation, and health care provider shortages can all affect one’s ability to obtain proper and efficient treatment.13 Rural areas may have a decreased availability of care services and providers compared with urban areas.20 Conversely, urban inner cities are faced with their own barriers to access. In urban cites, minority populations may face language barriers, a lack of cultural understanding, low educational attainment, a lack of social reinforcement for health-related behaviors and activities, and provider shortages which can limit appropriate access to treatment.13
Improving Patient Adherence in T2D
There is relatively broad agreement across scientific literature that medication adherence and/or persistence is far from uncommon in patients with T2D and may affect half this population at minimum.38,39 A magnitude of schemes, such as educational programs, disease management programs, intensive behavioral support, medication reminders, and special packaging, have been utilized to combat the lack of medication adherence across T2D; however, long-term, sustained improvements in rates of adherence have been difficult to achieve.38 The available body of data points to 6 key factors leading to nonadherence in T2D treatment: perceived treatment efficacy, hypoglycemia, treatment complexity and convenience, cost of treatment, medication beliefs, and physician trust.38
Poor medication adherence in T2D has been linked to negative health consequences, including increased mortality.38 A 2012 study examining managed care medical records by Jha et al noted that increased treatment adherence was associated a lower rate of hospital visits. The authors noted an approximately 13% lower probability of hospitalization for a patient adherent to treatment.15 A loss of adherence, however, lead to a nearly 15% increase in hospitalization in the following year.15 Additionally, greater medication adherence and improvements in measurable T2D treatment outcomes, such as A1C levels are linked.15
Drug combinations, such as a fixed-dose treatment, ease treatment burden by decreasing pill load which may have beneficial impacts on medication adherence.38,40 Currently, there are several fixed-dose combinations of agents available for the treatment of hyperglycemia in T2D.
Further, there is data to support initial combination therapy elicits more rapid attainment of glycemic goals.41,42 Matthews et al noted in their 2019 randomized, double-blind, parallel-group study of newly diagnosed patients with T2D that early combination therapy lead to a significant reduction in time to treatment failure as defined by A1C measurements and control (P <.0001).42
Further, a 2012 retrospective claims database analysis by Williams et al illustrated that patients on a fixed-dose combination had higher rates of achieving their A1C goals (61%) compared with step therapy (48%)(P <.001) or loose-dose combination (52%)(P = .015).43 This earlier attainment of optimal A1C levels due to combination therapy may facilitate decreased AEs due to lower dosing of individual drug components and curb dose intensifications.41
A collaboration between clinicians, diabetes educators, and pharmacists should center around optimizing the adherence of patients with T2D through clear communication and the incorporation of DSME and self-care behaviors while being mindful of patients’ treatment concerns and preferences.38,44
Summary
Clinicians should personalize goals for A1C control in patients with T2D based on a discussion of benefits and harms of drug therapy, patients’ preferences, impact of treatment burden, and associated costs of care. Over the past 2 decades, a greater proportion of individuals with T2D and their families have dealt with an increasing cost burden due to rising insurance premiums, drug prices, and health care costs.27
As health care systems and providers strive to provide optimal care and improve the health of their patients’ treatments must look outside of traditional clinical measurements but factor social and cultural norms.28 Novel treatment strategies bearing in mind social and economic factors impacting health should be integrated into patient care plans at all levels of the health care ecosystem.28 A greater utilization of pharmacists and electronic medical records and a decrease in associated treatment costs can increase patient medication adherence and in turn decrease patient burden.15
References
- American Diabetes Association. Economic costs of diabetes in the US in 2017. Diabetes Care. 2018;41(5):917‐928. doi: 10.2337/dci18-0007
- The cost of diabetes. American Diabetes Association website. Published March 2018. Accessed June 3, 2020. https://www.diabetes.org/resources/statistics/cost-diabetes#:~:text=Conclusion,that%20diabetes%20imposes%20on%20society
- Weng W, Tian Y, Kong SX, et al. Impact of atherosclerotic cardiovascular disease on healthcare resource utilization and costs in patients with type 2 diabetes mellitus in a real-world setting. Clin Diabetes Endocrinol. 2020;6:5. doi: 10.1186/s40842-019-0090-y
- Struijs JN, Baan CA, Schellevis FG, Westert GP, van den Bos GAM. Comorbidity in patients with diabetes mellitus: impact on medical health care utilization. BMC Health Serv Res. 2006;6:84. doi: 10.1186/1472-6963-6-84
- Teljeur C, Smith SM, Paul G, Kelly A, O’Dowd T. Multimorbidity in a cohort of patients with type 2 diabetes. Eur J Gen Pract. 2013;19(1):17-22. doi:10.3109/13814788.2012.714768
- National Diabetes Statistics Report 2020: estimates of diabetes and its burden in the United States. CDC website. Published February 14, 2020. Accessed May 7, 2020. https://www.cdc.gov/diabetes/data/statistics/statistics-report.html
- Lee TC, Glynn RJ, Peña JM, et al. Socioeconomic status and incident type 2 diabetes mellitus: data from the Women’s Health Study. PLoS One. 2011;6(12):e27670. doi: 10.1371/journal.pone.0027670
- Link CL, McKinlay JB. Disparities in the prevalence of diabetes: is it race/ethnicity or socioeconomic status? results from the Boston Area Community Health (BACH) Survey. Ethn Dis. 2009;19(3):288‐292.
- McLendon SF, Wood FG, Stanley N. Enhancing diabetes care through care coordination, telemedicine, and education: evaluation of a rural pilot program. Public Health Nurs. 2019;36(3):310‐320. doi: 10.1111/phn.12601
- American Diabetes Association. 1. Improving care and promoting health in populations: Standards of Medical Care in Diabetes-2020. Diabetes Care. 2018;41(suppl 1):S7‐S12. doi: 10.2337/dc18-S001
- Sood A, Watts SA, Johnson JK, Hirth S, Aron DC. Telemedicine consultation for patients with diabetes mellitus: a cluster randomised controlled trial. J Telemed Telecare. 2018;24(6):385‐391. doi: 10.1177/1357633X17704346
- von Storch K, Graaf E, Wunderlich M, Rietz C, Polidori MC, Woopen C. Telemedicine-assisted self-management program for type 2 diabetes patients. Diabetes Technol Ther. 2019;21(9):514‐521. doi: 10.1089/dia.2019.0056
- Shea S, Weinstock RS, Teresi JA, et al; IDEATel Consortium. A randomized trial comparing telemedicine case management with usual care in older, ethnically diverse, medically underserved patients with diabetes mellitus: 5 year results of the IDEATel study. J Am Med Inform Assoc. 2009;16(4):446‐456. doi: 10.1197/jamia.M3157
- Izquierdo RE, Knudson PE, Meyer S, Kearns J, Ploutz-Snyder R, Weinstock RS. A comparison of diabetes education administered through telemedicine versus in person. Diabetes Care. 2003;26(4):1002‐1007. doi: 10.2337/diacare.26.4.1002
- Jha AK, Aubert RE, Yao J, Teagarden JR, Epstein RS. Greater adherence to diabetes drugs is linked to less hospital use and could save nearly $5 billion annually. Health Aff (Millwood). 2012;31(8):1836‐1846. doi: 10.1377/hlthaff.2011.1198
- Duncan I, Birkmeyer C, Coughlin S, Li QE, Sherr D, Boren S. Assessing the value of diabetes education. Diabetes Educ. 2009;35(5):752‐760. doi: 10.1177/0145721709343609
- Chester B, Stanely WG, Geetha T. Quick guide to type 2 diabetes self-management education: creating an interdisciplinary diabetes management team. Diabetes Metab Syndr Obes. 2018;11:641‐645. doi: 10.2147/DMSO.S178556
- Beck J, Greenwood DA, Blanton L, et al; 2017 Standards Revision Task Force. 2017 National Standards for Diabetes Self-Management Education and Support [erratum in Diabetes Educ. 2017;43(6):650]. Diabetes Educ. 2017;43(5):449‐464. doi: 10.1177/0145721717722968
- Peyrot M, Rubin RR. Access to diabetes self-management education. Diabetes Educ. 2008;34(1):90‐97. doi: 10.1177/0145721707312399
- Siminerio LM, Piatt G, Zgibor JC. Implementing the chronic care model for improvements in diabetes care and education in a rural primary care practice. Diabetes Educ. 2005;31(2):225‐234. doi: 10.1177/0145721705275325
- Powers MA, Bardsley J, Cypress M, et al. Diabetes self-management education and support in type 2 diabetes: a joint position statement of the American Diabetes Association, the American Association of Diabetes Educators, and the Academy of Nutrition and Dietetics. J Acad Nutr Diet. 2015;115(8):1323‐1334. doi: 10.1016/j.jand.2015.05.012
- Inzucchi SE, Bergenstal RM, Buse JB, et al. Management of hyperglycemia in type 2 diabetes, 2015: a patient-centered approach: update to a position statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care. 2015;38(1):140‐149. doi: 10.2337/dc14-2441
- Lopez JMS, Macomson B, Ektare V, Patel D, Botteman M. Evaluating drug cost per response with SGLT2 inhibitors in patients with type 2 diabetes mellitus. Am Health Drug Benefits. 2015;8(6):309‐318.
- Williams SA, Buysman EK, Hulbert EM, Bergeson JG, Zhang B, Graham J. Hemoglobin A1c outcomes and health care resource use in type 2 diabetes mellitus patients treated with combination oral antidiabetic drugs through step therapy and loose-dose and fixed-dose combinations. Manag Care. 2012;21(7):40‐48.
- Ryan PB, Buse JB, Schuemie MJ, et al. Comparative effectiveness of canagliflozin, SGLT2 inhibitors and non-SGLT2 inhibitors on the risk of hospitalization for heart failure and amputation in patients with type 2 diabetes mellitus: A real-world meta-analysis of 4 observational databases (OBSERVE-4D). Diabetes Obes Metab. 2018;20(11):2585-2597. doi:10.1111/dom.13424
- Chen YW, Voelker J, Tunceli O, Pericone CD, Bookhart B, Durkin M. Real-world comparison of hospitalization costs for heart failure in type 2 diabetes mellitus patients with established cardiovascular disease treated with canagliflozin versus other antihyperglycemic agents. J Med Econ. 2020;23(4):401-406. doi:10.1080/13696998.2019.1693384
- American Diabetes Association. 9. Pharmacologic approaches to glycemic treatment: Standards of Medical Care in Diabetes-2020. Diabetes Care. 2020; 43(supp 1):S98–S110. doi: 10.2337/dc20-S009.
- Quiñones AR, Talavera GA, Castañeda SF, Saha S. Interventions that reach into communities—promising directions for reducing racial and ethnic disparities in healthcare. J Racial Ethn Health Disparities. 2015;2(3):336‐340. doi: 10.1007/s40615-014-0078-3
- Nwasuruba C, Khan M, Egede LE. Racial/ethnic differences in multiple self-care behaviors in adults with diabetes. J Gen Intern Med. 2007;22(1):115‐120. doi: 10.1007/s11606-007-0120-9
- Assari S, Moghani Lankarani M, Piette JD, Aikens JE. Socioeconomic status and glycemic control in type 2 diabetes; race by gender differences. Healthcare (Basel). 2017;5(4):83. doi: 10.3390/healthcare5040083
- Liese AD, Ma X, Reid L, et al. Health care access and glycemic control in youth and young adults with type 1 and type 2 diabetes in South Carolina. Pediatr Diabetes. 2019;20(3):321-329. doi: 10.1111/pedi.12822
- Arpey NC, Gaglioti AH, Rosenbaum ME. How socioeconomic status affects patient perceptions of health care: a qualitative study. J Prim Care Community Health. 2017;8(3):169-175. doi: 10.1177/2150131917697439
- Henk HJ, Lopez JMS, Bookhart BK. Novel type 2 diabetes medication access and effect of patient cost sharing. J Manag Care Spec Pharm. 2018;24(9):847‐855. doi: 10.18553/jmcp.2018.24.9.847
- Thornton Snider J, Seabury S, Lopez J, McKenzie S, Goldman DP. Impact of type 2 diabetes medication cost sharing on patient outcomes and health plan costs. Am J Manag Care. 2016;22(6):433‐440.
- Greenapple R. Review of strategies to enhance outcomes for patients with type 2 diabetes: payers’ perspective. Am Health Drug Benefits. 2011;4(6):377‐386.
- Fendrick AM. Value-based insurance design for diabetes mellitus: approaches to optimal pharmacoeconomic implementation. Am J Manag Care. 2010;16(supp 11):S314-S322.
- Nash DB, Skoufalos A, Harris D. Achieving a patient-centered, value-based system of diabetes care in the United States: report on a national stakeholder summit. Popul Health Manag. 2018;21(1):20‐23. doi: 10.1089/pop.2017.0131
- Polonsky WH, Henry RR. Poor medication adherence in type 2 diabetes: recognizing the scope of the problem and its key contributors. Patient Prefer Adherence. 2016;10:1299‐1307. doi: 10.2147/PPA.S106821
- Kirkman MS, Rowan-Martin MT, Levin R, et al. Determinants of adherence to diabetes medications: findings from a large pharmacy claims database. Diabetes Care. 2015;38(4):604‐609. doi: 10.2337/dc14-2098
- García-Pérez LE, Alvarez M, Dilla T, Gil-Guillén V, Orozco-Beltrán D. Adherence to therapies in patients with type 2 diabetes. Diabetes Ther. 2013;4(2):175‐194. doi: 10.1007/s13300-013-0034-y
- Phung OJ, Sobieraj DM, Engel SS, Rajpathak SN. Early combination therapy for the treatment of type 2 diabetes mellitus: systematic review and meta-analysis. Diabetes Obes Metab. 2014;16(5):410‐417. doi: 10.1111/dom.12233
- Matthews DR, Paldánius PM, Proot P, et al; VERIFY study group. Glycaemic durability of an early combination therapy with vildagliptin and metformin versus sequential metformin monotherapy in newly diagnosed type 2 diabetes (VERIFY): a 5-year, multicentre, randomised, double-blind trial. Lancet. 2019;394(10208):1519‐1529. doi: 10.1016/S0140-6736(19)32131-2
- Williams SA, Buysman EK, Hulbert EM, Bergeson JG, Zhang B, Graham J. Hemoglobin A1c outcomes and health care resource use in type 2 diabetes mellitus patients treated with combination oral antidiabetic drugs through step therapy and loose-dose and fixed-dose combinations. Manag Care. 2012;21(7):40‐48.
- Egede LE, Gebregziabher M, Echols C, Lynch CP. Longitudinal effects of medication nonadherence on glycemic control. Ann Pharmacother. 2014;48(5):562‐570. doi: 10.1177/1060028014526362
Articles in this issue
Advertisement
Related Content




{kind=link}
{kind=link}
{kind=link}
Advertisement
Advertisement
Trending on AJMC
1
FDA Approves First Oral Carbapenem Antibiotic for Complicated UTIs
2
EHA 2026 Had Something for Everyone, From Pediatric Practitioners to “Myeloma Maniacs”
3
Fourteen Years of HIV PrEP: How New Innovations Build on Decades of Progress in HIV
4
5 Ongoing Clinical Trials in Myeloproliferative Neoplasms
5