ARIKAYCE ® (amikacin liposome inhalation suspension) Formulary Central
SPONSORED CONTENT
To request additional information, email medicalinformation@insmed.com or
call (844) 446-7633.
WARNING: RISK OF INCREASED RESPIRATORY ADVERSE REACTIONS
Hypersensitivity Pneumonitis has been reported with the use of ARIKAYCE in the clinical trials. Hypersensitivity pneumonitis (reported as allergic alveolitis, pneumonitis, interstitial lung disease, allergic reaction to ARIKAYCE) was reported at a higher frequency in patients treated with ARIKAYCE plus background regimen (3.1%) compared to patients treated with a background regimen alone (0%). Most patients with hypersensitivity pneumonitis discontinued treatment with ARIKAYCE and received treatment with corticosteroids. If hypersensitivity pneumonitis occurs, discontinue ARIKAYCE and manage patients as medically appropriate.
Hemoptysis has been reported with the use of ARIKAYCE in the clinical trials. Hemoptysis was reported at a higher frequency in patients treated with ARIKAYCE plus background regimen (17.9%) compared to patients treated with a background regimen alone (12.5%). If hemoptysis occurs, manage patients as medically appropriate.
Bronchospasm has been reported with the use of ARIKAYCE in the clinical trials. Bronchospasm (reported as asthma, bronchial hyperreactivity, bronchospasm, dyspnea, dyspnea exertional, prolonged expiration, throat tightness, wheezing) was reported at a higher frequency in patients treated with ARIKAYCE plus background regimen (28.7%) compared to patients treated with a background regimen alone (10.7 %). If bronchospasm occurs during the use of ARIKAYCE, treat patients as medically appropriate.
Exacerbations of underlying pulmonary disease has been reported with the use of ARIKAYCE in the clinical trials. Exacerbations of underlying pulmonary disease (reported as chronic obstructive pulmonary disease (COPD), infective exacerbation of COPD, infective exacerbation of bronchiectasis) have been reported at a higher frequency in patients treated with ARIKAYCE plus background regimen (14.8%) compared to patients treated with background regimen alone (9.8%). If exacerbations of underlying pulmonary disease occur during the use of ARIKAYCE, treat patients as medically appropriate.
Ototoxicity has been reported with the use of ARIKAYCE in the clinical trials. Ototoxicity (including deafness, dizziness, presyncope, tinnitus, and vertigo) were reported with a higher frequency in patients treated with ARIKAYCE plus background regimen (17 %) compared to patients treated with background regimen alone (9.8%). This was primarily driven by tinnitus (7.6% in ARIKAYCE plus background regimen vs 0.9% in the background regimen alone arm) and dizziness (6.3% in ARIKAYCE plus background regimen vs 2.7% in the background regimen alone arm). Closely monitor patients with known or suspected auditory or vestibular dysfunction during treatment with ARIKAYCE. If ototoxicity occurs, manage patients as medically appropriate, including potentially discontinuing ARIKAYCE.
Nephrotoxicity was observed during the clinical trials of ARIKAYCE in patients with MAC lung disease but not at a higher frequency than background regimen alone. Nephrotoxicity has been associated with the aminoglycosides. Close monitoring of patients with known or suspected renal dysfunction may be needed when prescribing ARIKAYCE.
Neuromuscular Blockade: Patients with neuromuscular disorders were not enrolled in ARIKAYCE clinical trials. Patients with known or suspected neuromuscular disorders, such as myasthenia gravis, should be closely monitored since aminoglycosides may aggravate muscle weakness by blocking the release of acetylcholine at neuromuscular junctions.
Embryo-Fetal Toxicity: Aminoglycosides can cause fetal harm when administered to a pregnant woman. Aminoglycosides, including ARIKAYCE, may be associated with total, irreversible, bilateral congenital deafness in pediatric patients exposed in utero. Patients who use ARIKAYCE during pregnancy, or become pregnant while taking ARIKAYCE should be apprised of the potential hazard to the fetus.
Contraindications: ARIKAYCE is contraindicated in patients with known hypersensitivity to any aminoglycoside.
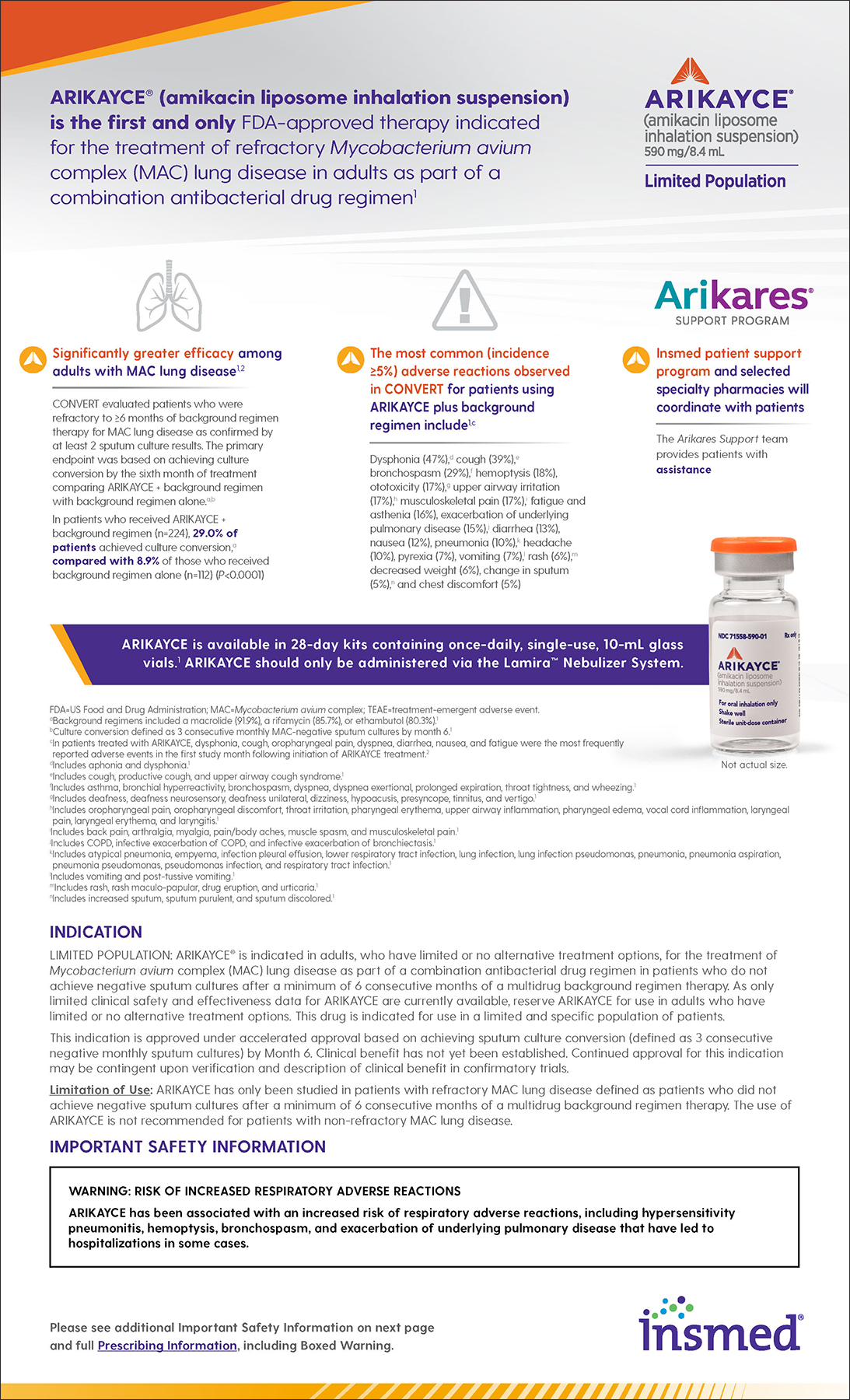
Most Common Adverse Reactions: The most common adverse reactions in Trial 1 at an incidence ≥5% for patients using ARIKAYCE plus background regimen compared to patients treated with background regimen alone were dysphonia (47% vs 1%), cough (39% vs 17%), bronchospasm (29% vs 11%), hemoptysis (18% vs 13%), ototoxicity (17% vs 10%), upper airway irritation (17% vs 2%), musculoskeletal pain (17% vs 8%), fatigue and asthenia (16% vs 10%), exacerbation of underlying pulmonary disease (15% vs 10%), diarrhea (13% vs 5%), nausea (12% vs 4%), pneumonia (10% vs 8%), headache (10% vs 5%), pyrexia (7% vs 5%), vomiting (7% vs 4%), rash (6% vs 2%), decreased weight (6% vs 1%), change in sputum (5% vs 1%), and chest discomfort (5% vs 3%).
Drug Interactions: Avoid concomitant use of ARIKAYCE with medications associated with neurotoxicity, nephrotoxicity, and ototoxicity. Some diuretics can enhance aminoglycoside toxicity by altering aminoglycoside concentrations in serum and tissue. Avoid concomitant use of ARIKAYCE with ethacrynic acid, furosemide, urea, or intravenous mannitol.
Overdosage: Adverse reactions specifically associated with overdose of ARIKAYCE have not been identified. Acute toxicity should be treated with immediate withdrawal of ARIKAYCE, and baseline tests of renal function should be undertaken. Hemodialysis may be helpful in removing amikacin from the body. In all cases of suspected overdosage, physicians should contact the Regional Poison Control Center for information about effective treatment.
Insmed and ARIKAYCE are trademarks of Insmed Incorporated. PP-ARIK-US-00039