This site is sponsored by Genentech and is solely intended for financial analysis by population health decision makers.

The role of HEMLIBRA® (emicizumab‑kxwh) in hemophilia A management for patients with or without FVIII inhibitors
Prophylaxis treatment differentiators and economic considerations
Hemlibra Key Features
Treatment landscape differentiators
- HEMLIBRA has the largest pivotal clinical trial program in hemophilia A for patients with and without FVIII inhibitors1
- Outside of the HAVEN 1–4 pivotal trials, HEMLIBRA has also been widely studied in the real-world setting, leading to a total of more than 190 real-world publications1*†
- HEMLIBRA is priced at the lowest WAC compared to all leading alternatives within the therapeutic category1
- HEMLIBRA has been proven and trusted by the community for 7+ years; over 30,000 patients
worldwide‡ and over 8600 patients in the US have been treated with
HEMLIBRA1,2§
- Approved in 2017 for adults and children with hemophilia A with FVIII inhibitors3
- Approved in 2018 for adults and children with hemophilia A with or without FVIII inhibitors4
- HEMLIBRA is the #1 prescribed prophylaxis in the US for people with hemophilia A without
FVIII inhibitors according to IQVIA claims data (various insurance plan types) from
Dec’23-Nov’24 (Refreshed Feb’25), accounting for prophylaxis use in the US1,5
- Highest market share among prophylactic treatments for both indications: 61% for noninhibitor and 80% for inhibitor [based on IQVIA claims data (Q1 2023 claims not mature) and a Genentech internal analysis (Q1 2023)]1
- HEMLIBRA is the first subcutaneous injection prophylactic treatment for hemophilia A, with or without FVIII inhibitors, and the first therapeutic bispecific monoclonal antibody that bridges FIXa and FX, enabling the coagulation cascade to proceed without the need to replace FVIII1,5
- According to the National Bleeding Disorder Foundation’s (NBDF’s) Medical and Scientific Advisory Council (MASAC) guidelines, when making treatment decisions for people with hemophilia A (PwHA), healthcare providers should discuss HEMLIBRA as an option for individuals of any age or severity, with or without inhibitors. Approved for all PwHA, HEMLIBRA is recommended as a first-line treatment for those with FVIII inhibitors. It may also be considered for infants anytime after birth due to the risk of intracranial hemorrhage before starting FVIII prophylaxis. Both HEMLIBRA and FVIII prophylaxis should be considered therapeutic options for this age6
*A literature search of PubMed, ProQuest, and major hemophilia congress abstract books was conducted on September 15, 2022. Reports describing efficacy, safety, or surgical outcomes related to HEMLIBRA in the real-world setting were selected. Some publications may contain duplicate patient participants who were assessed in more than one study.
†Publications include journal articles and congress presentations.
‡Number of patients with hemophilia A treated with HEMLIBRA worldwide as of June 2025.1
§Number of patients with hemophilia A treated with HEMLIBRA in the US as of August 2025.1
Dosage
- HEMLIBRA offers 6 different vial strengths, providing more options to meet the needs of
appropriate members with hemophilia A5
- The selection of maintenance dose should be based on healthcare provider preference with consideration of regimens that may increase patient adherence5
Indication
HEMLIBRA is indicated for routine prophylaxis to prevent or reduce the frequency of bleeding episodes in adult and pediatric patients ages newborn and older with hemophilia A with or without factor VIII inhibitors.
Important Safety Information
Boxed WARNING: THROMBOTIC MICROANGIOPATHY and THROMBOEMBOLISM
Cases of thrombotic microangiopathy and thrombotic events were reported when on average a cumulative amount of >100 U/kg/24 hours of activated prothrombin complex concentrate (aPCC) was administered for 24 hours or more to patients receiving HEMLIBRA prophylaxis. Monitor for the development of thrombotic microangiopathy and thrombotic events if aPCC is administered. Discontinue aPCC and suspend dosing of HEMLIBRA if symptoms occur.
Please see additional Important Safety Information, including Boxed WARNING, and the HEMLIBRA full Prescribing Information.
Hemlibra clinical trial overview
Clinical development program
HEMLIBRA has 10+ years of clinical trial experience in ~800 patients with hemophilia A, and has been studied across 9 Phase 3 clinical trials. The population studied included infants; previously untreated and minimally treated patients; pediatrics and adults; mild, moderate, and severe patients; and patients with and without inhibitors.5,7‑12
In 4 pivotal clinical trials, HEMLIBRA demonstrated reductions in treated bleeds across diverse populations with hemophilia A
HAVEN 1
included adolescent and adult patients with FVIII inhibitors.II Patients receiving HEMLIBRA 1.5 mg/kg QW (n=35) had a mean annualized bleed rate (ABR) of 2.9 (95% CI: 1.7; 5.0) compared to 23.3 (95% CI: 12.3; 43.9) in those with no prophylaxis (n=18). The median treatment durations were 29.3 weeks (HEMLIBRA) and 24 weeks (no prophylaxis).5
HAVEN 2
included pediatric patients with FVIII inhibitors receiving HEMLIBRA 1.5 mg/kg QW (n=59), with a mean ABR of 0.3 (95% CI: 0.1; 0.5) and a median treatment duration of 29.6 weeks.5¶
HAVEN 3
included adolescent and adult patients without FVIII inhibitors.II Patients receiving HEMLIBRA 1.5 mg/kg QW (n=36) had a mean ABR of 1.5 (95% CI: 0.9; 2.5), while those on HEMLIBRA 3 mg/kg Q2W (n=35) had an ABR of 1.3 (95% CI: 0.8; 2.3). The no prophylaxis group (n=18) had a mean ABR of 38.2 (95% CI: 22.9; 63.8). Median treatment durations were 29.6 weeks, 31.3 weeks, and 24 weeks, respectively.5
HAVEN 4
included adolescent and adult patients with or without FVIII inhibitorsII receiving HEMLIBRA 6 mg/kg Q4W (n=41), with a mean ABR of 2.4 (95% CI: 1.4; 4.3) over a median treatment duration of 25.6 weeks.5
Based on pooled data from HAVEN 1–4 and a dose-finding trial, the most common adverse events in ≥10% of patients included injection site reactions (ISRs), headaches, and arthralgia.5
IIAdolescent patients were defined as individuals aged ≥12 years and <18
years.5
¶Pediatric patients were defined as individuals aged <12 years.5
The details of HAVEN 1–4 can be found in the HEMLIBRA Package Insert at https://www.gene.com/download/pdf/
Economic considerations
These healthcare economic materials were prepared pursuant to FD&C Act Sec. 502(a) standards. They are intended solely for use with payers, formulary committees, or other similar entities with knowledge and expertise in the area of healthcare economic analysis to facilitate drug selection decisions for coverage or reimbursement. These materials are not intended to be used by healthcare practitioners for the purpose of making individual patient prescribing decisions.
WAC pricing
For an average plan member with hemophilia A, HEMLIBRA is less expensive annually on a WAC basis (and comparable on an ASP basis) when compared with leading EHL and SHL FVIII products (as of January 2025). The annual WAC of leading prophylaxis therapies are as follows1:
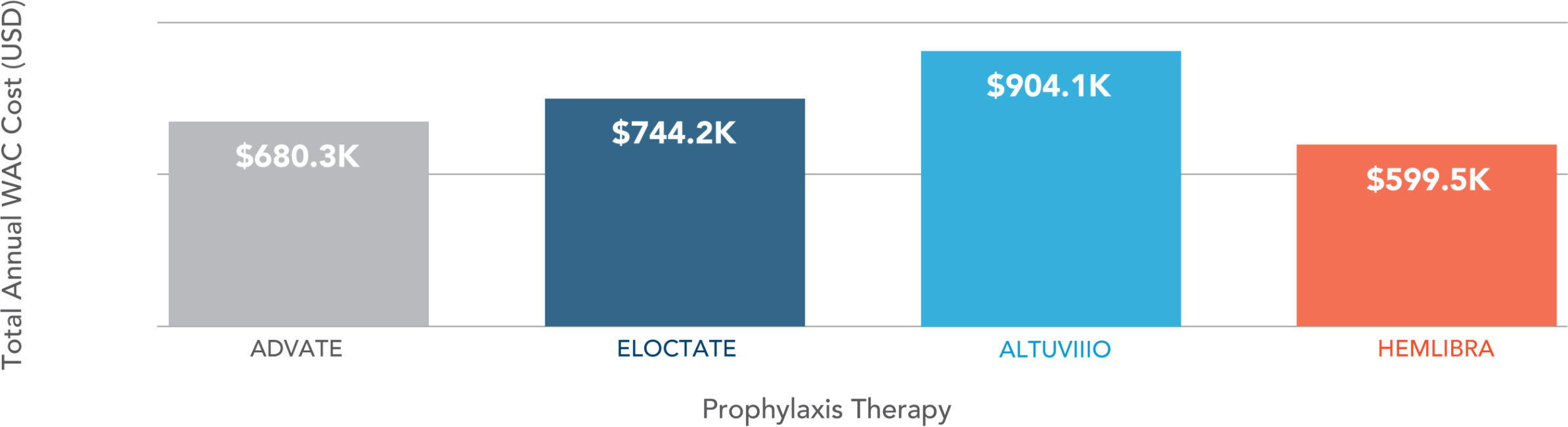
KEY ASSUMPTIONS
Annualized (52.14-week) average WAC for prophylaxis with Advate®, Eloctate®, Altuviiio®, and HEMLIBRA in a patient weighing 63.4 kg.
Based on average US dosing data from the American Thrombosis and Hemostasis Network (ATHN), the doses of 118.2 IU/kg per week for Advate, 111.2 IU/kg per week for Eloctate, and 50 IU/kg for Altuviiio were applied.
Cost of drug can be highly variable depending on several factors, including dosing schedule and disease severity. Additionally, the actual acquisition cost paid by purchasers may vary and may or may not include discounts or other reductions in price.
HEMLIBRA costs an additional ~$46K for an average patient in Year 1 due to the loading dose.
No comparative safety or efficacy conclusions can be drawn from the pricing information. The drugs or regimens presented are not interchangeable or therapeutically equivalent.
REAL-WORLD HCRU IN THE US PRE- AND POST-HEMLIBRA
The following information includes data based on an analysis performed by Genentech. This study is intended for informational purposes only.
A retrospective, observational cohort study examined HCRU before and after starting HEMLIBRA using US adjudicated health plan claims data from IQVIA PharMetrics® Plus, and included patients (N=472) who received ≥1 HEMLIBRA prescription fill between November 1, 2017, and June 30, 2023. The mean age of participants was 24.7 years (SD: 17.3 years), 99% were male, and 64% were aged less than 31 years.13
HCRU was evaluated during the 12 months pre- and post-HEMLIBRA initiation, including all-cause inpatient hospitalizations; outpatient hospital, ER, and physician office visits; and FVIII prescription fills.13
In the 12 months following treatment initiation relative to the 12 months prior, it was observed that patients in the overall study population who initiated HEMLIBRA had fewer inpatient hospitalizations, outpatient hospital visits, and ER visits. FVIII prescription fills were also significantly reduced post-HEMLIBRA (P<0.001).13
Inpatient hospitalizations, outpatient hospital visits, ER visits, and FVIII fills among PwHA pre- and post-HEMLIBRA
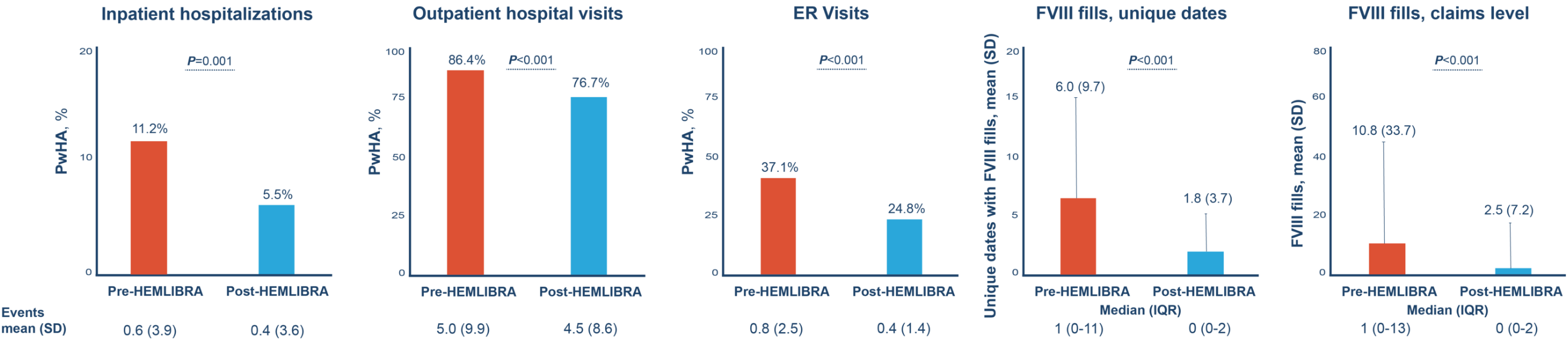
- There was reduced variability in HCRU outcomes after initiating HEMLIBRA13
- Pre-post difference in number of physician office visits was not significant (P>0.05)13
- While the proportion of patients with hospitalizations and the number of hospitalizations were numerically reduced across all age groups, the reductions were only statistically significant in the <31-year age groups and not in the ≥31-year age group13
- Reductions in all measures of HCRU were observed post-HEMLIBRA regardless of prior hemophilia A treatment; however, it was only statistically significant in the treatment‑experienced patients and not in previously untreated PwHA13
- Results were consistent across commercial, Medicare, and Medicaid insurance types13
Limitations
This study population primarily comprised of PwHA who had commercial insurance, so results may not be generalizable to populations with other insurance types. As a well-known limitation of the use of claims data, this study relies on the accuracy of administrative claims data.13
COST-EFFECTIVENESS ANALYSIS
The following information includes data based on an analysis performed by Genentech. This study is intended for informational purposes only.
A 2023 cost-effectiveness analysis based on a Markov Model evaluated prophylaxis treatments for adult patients with hemophilia A without inhibitors in the US and included HEMLIBRA, Altuviiio, Advate, and Eloctate.14
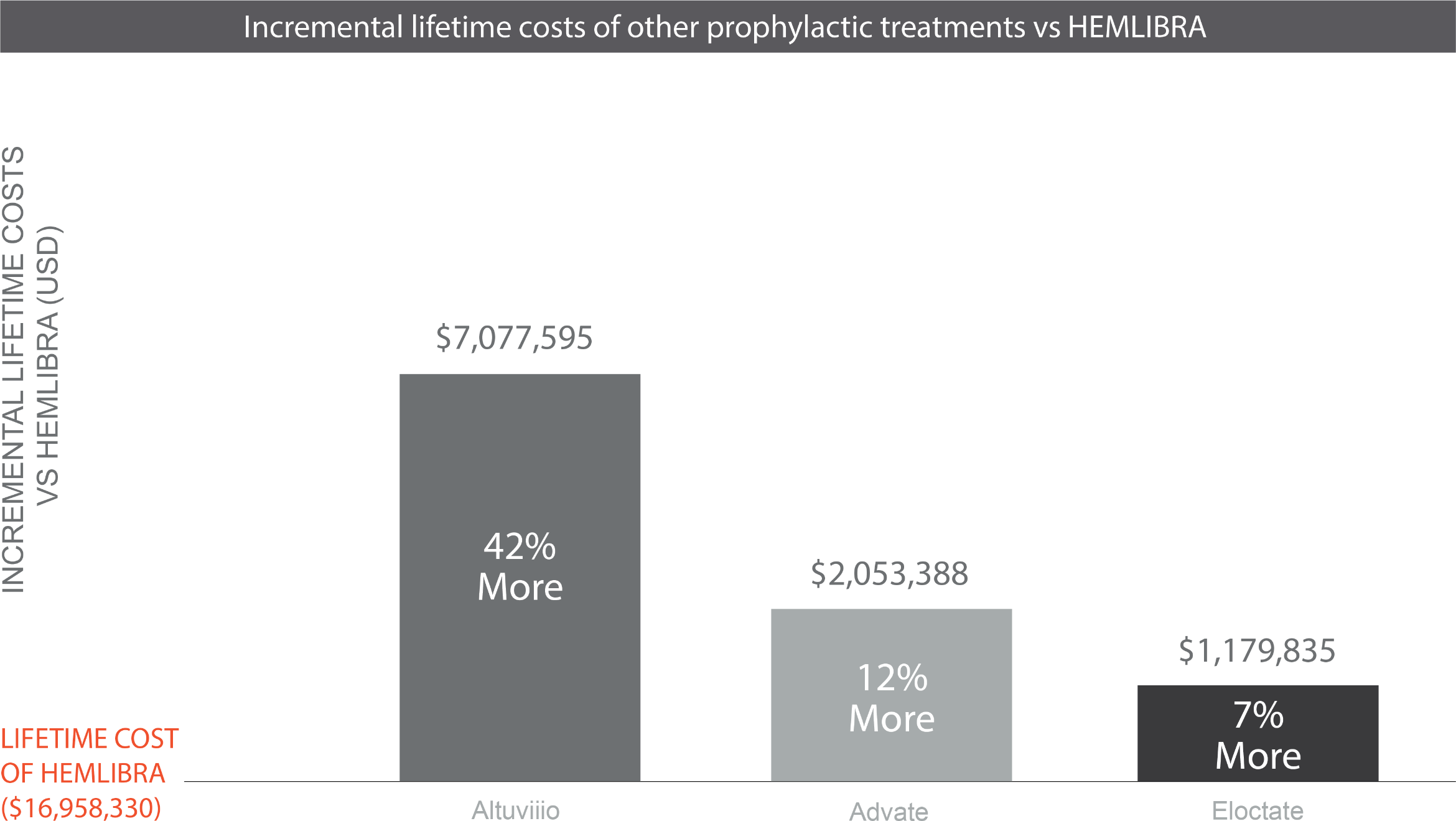
Over a patient’s lifetime1,14:
- HEMLIBRA was shown to be cost-saving as a prophylactic treatment for PwHA without inhibitors when compared to Altuviiio, Advate, and Eloctate
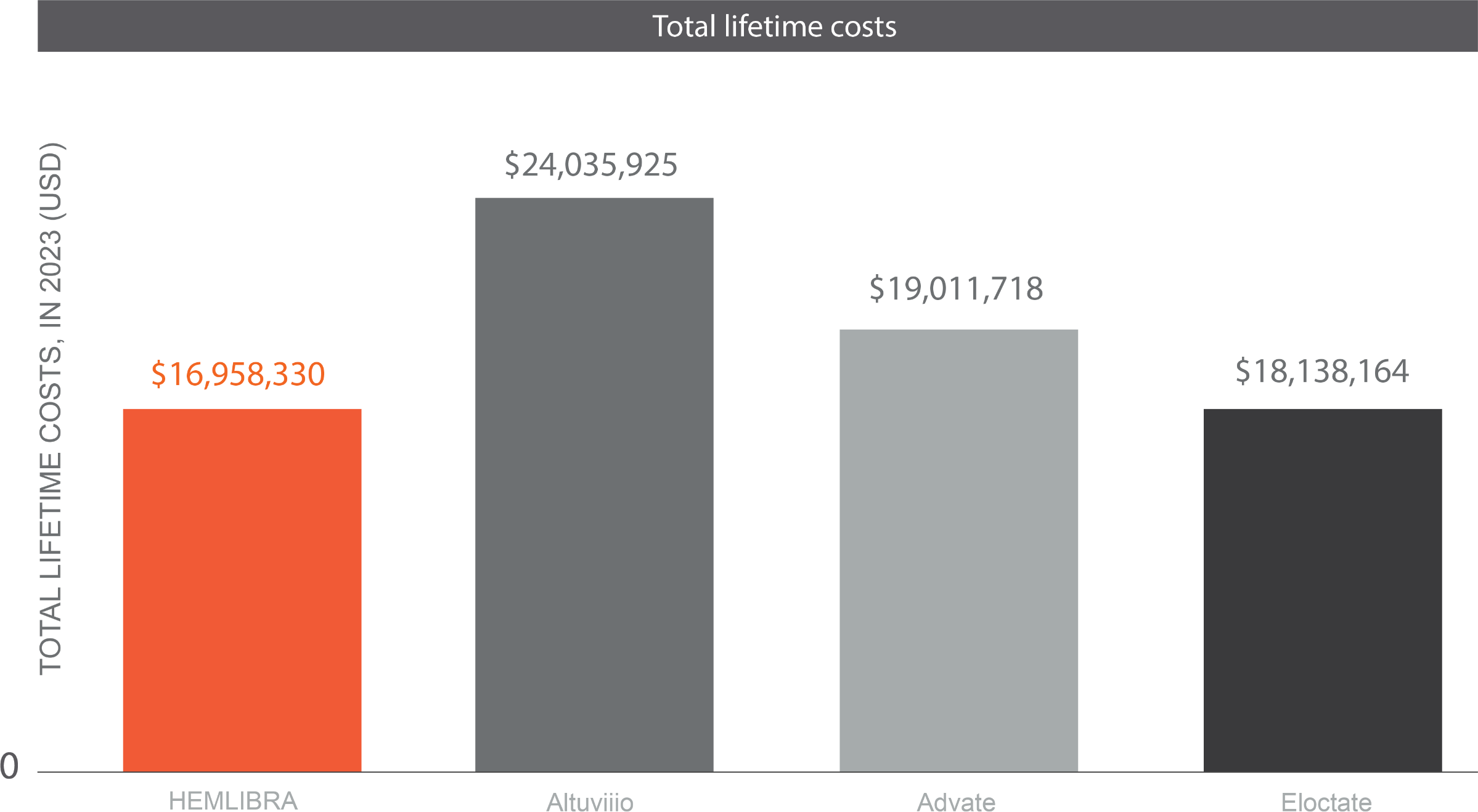
- HEMLIBRA had the highest quality-adjusted life-years (QALYs) relative to all the products in this study14
- Results were robust to sensitivity analyses14
KEY ASSUMPTIONS
- The conceptual model captures quality of life by disease severity, where treatment choice
impacts
the disease severity1
- While trial patients were included if they had a severe phenotype (defined per trial
protocols that included
FVIII levels and annual bleed rate), this model determined severity by FVIII
levels1:
- <1% severe
- 1–5% moderate
- 5–40% mild
- >40% normal clotting function
- Treatments affect the probability and duration of time that a PwHA lives in a severity state1
- While trial patients were included if they had a severe phenotype (defined per trial
protocols that included
FVIII levels and annual bleed rate), this model determined severity by FVIII
levels1:
- Age weights were not applied to utilities; a QALY is valued the same at all ages1
- Health state utilities for mild, moderate, and severe hemophilia include impacts of bleeding events1
- Drug costs were estimated from WAC; ASP was not used since data on ASP of the new products were not available1
- Mortality differences between products have not been observed; current evidence from the Centers for Disease Control and Prevention was used, which indicates that mortality for persons with hemophilia A is the same as age-matched individuals1
- Adherence to HEMLIBRA was 97%, SHL and EHL factor adherence was 84% (based on real-world evidence), and Altuviiio adherence was assumed to be an average of the two, 91%; modeling this involved a pharmacokinetics-based assumption that nonadherent HEMLIBRA patients would experience a moderate disease state while nonadherent factor patients would experience a severe disease state1
- All bleeds use SHL factor products, regardless of prophylaxis1
Limitations
Lack of head-to-head data; differences in trial populations across products may have impacted assessment of costs and effectiveness; discounting and rebates were not accounted in the price of products.14
Adherence and persistence in a retrospective study
The following information includes data based on an analysis performed by Genentech. This study is intended for informational purposes only.
A retrospective, observational study analyzed real-world adherence and persistence to HEMLIBRA prophylaxis among 280 PwHA using US health plan claims data from IQVIA PharMetrics Plus. Persistence was calculated as the proportion of patients continuing HEMLIBRA treatment within 12 months of initial fill, where discontinuation was defined as a treatment gap of at least 60 days. Adherence was defined as having at least 80% proportion of days covered and calculated during the 12-month period after initial fill of HEMLIBRA.1,15
- Over a 12-month period, 85% of patients remained persistent with HEMLIBRA and 76% were adherent1,15
- Among adherent patients, less than half (43%) had any FVIII claims during the 1-year follow-up period. The mean (SD) number of FVIII claims was 1.14 (2.04) during the follow-up1,15
Limitations
Claims data only captured medications that were dispensed but does not provide information on whether the patient took the medication as intended. Study population was largely commercially insured.1,15
Literature searches on Embase from 2023 onward identified 1 US cost-effectiveness model comparing HEMLIBRA and FVIII; 1 claims-based analysis of HEMLIBRA adherence or persistence; and 2 US analyses of HCRU (only one of which is described here; an additional HCP survey showed no conflicting results).13-16
Additional clinical trial data
HAVEN 7, THE FIRST TRIAL OF HEMLIBRA DEDICATED TO INFANTS12
According to NBDF-MASAC, “prophylaxis should be initiated at an early age, ideally before age 3 years and prior to the second joint bleed; prophylaxis may be considered within the first 6 months of life to reduce occurrence of intracranial hemorrhage.”17
Treatment with intravenous FVIII can have challenges in infants due to potential of venous access difficulties, risks associated with central venous access devices, and the likelihood of inhibitor development.17
HAVEN 7 is the first clinical trial of HEMLIBRA dedicated to infants (≤12 months of age) with severe hemophilia A without FVIII inhibitors. After the first 4 weekly loading doses, infants received HEMLIBRA Q2W for one year, and then had the option to continue Q2W or switch to QW or Q4W dosing.12
The primary analysis involved 55 infants, with ages at enrollment ranging from 9 days to 11 months and 30 days. Of these, 25 (45.5%) were previously untreated patients, and 30 (54.5%) were minimally treated (patients with ≤5 exposure days to FVIII). The model-based ABR for treated bleeds was 0.4 (95% CI: 0.3; 0.6), and all bleeds were traumatic. 55% of infants had zero treated bleeds. The median follow-up period was 100.3 weeks (range: 52-118 weeks).12
No new safety concerns were found in the HAVEN 7 study. No intracranial hemorrhage, thromboembolic events (TEs), thrombotic microangiopathies (TMAs), or deaths were reported. All patients experienced an AE (631 AEs in total); nine patients had ≥1 AE related to HEMLIBRA (all Grade 1 ISRs). Sixteen patients experienced a total of 30 serious AEs; none of them related to HEMLIBRA. Two patients developed FVIII inhibitors.12
Limitations
HAVEN 7 was a single-arm, open-label study. Patients with current active severe bleeds, such as intracranial hemorrhages, were not included. These data are a descriptive analysis and therefore should be interpreted with caution.12
HAVEN 1–4 long-term analysis
The median efficacy period of HEMLIBRA across HAVEN 1–4 trials was 120.4 weeks (IQR: 89–164.4). Out of the 400 participants assigned to the study treatment, 399 received the treatment.18
Across HAVEN 1–4 studies, the model-based ABR for treated bleeds was 1.4 (95% CI: 1.1; 1.7). The proportion of patients with zero treated bleeds was 70.8% (n=391) during the first 24-week interval and remained above 80% (n=374) during subsequent 24-week intervals until week 144. Target joint resolution, defined as ≤2 bleeding events in a 52-week period in a joint previously defined as a target joint, was achieved in 95.1% of target joints across HAVEN 1–4.18
Long-term safety was consistent with safety findings from the primary analysis. No new safety concerns were identified. Out of 399 people who received HEMLIBRA, 381 (96%) reported ≥1 adverse event during a median duration exposure of 130.3 weeks. The most common treatment-related adverse reaction was ISR (107/399; 27%). The majority of all ISRs (treatment-related or not) were mild (104/111; 94%) and occurred during the first 24 weeks (93/111; 84%). One hundred forty-four serious side effects occurred in 93 people. Six people had treatment-related serious side effects. There were 3 TMAs and 4 TEs. All 3 TMAs and 2 of 4 TEs were associated with concomitant aPCC use and were previously reported in HAVEN 1.18
Limitations
This analysis is a descriptive study and should be interpreted with caution. Data for each period should be looked at individually and not over time. Long-term studies face challenges such as reporting fatigue, dropout, and variability across studies. Patient numbers declined over time, as many transitioned to commercial HEMLIBRA. Patients were excluded from further analysis once they switched. Some patients also discontinued for other reasons.18
Important safety information
Indication
HEMLIBRA is indicated for routine prophylaxis to prevent or reduce the frequency of bleeding episodes in adult and pediatric patients ages newborn and older with hemophilia A with or without factor VIII inhibitors.
Important Safety Information
Boxed WARNING: THROMBOTIC MICROANGIOPATHY and THROMBOEMBOLISM
Cases of thrombotic microangiopathy and thrombotic events were reported when on average a cumulative amount of >100 U/kg/24 hours of activated prothrombin complex concentrate (aPCC) was administered for 24 hours or more to patients receiving HEMLIBRA prophylaxis. Monitor for the development of thrombotic microangiopathy and thrombotic events if aPCC is administered. Discontinue aPCC and suspend dosing of HEMLIBRA if symptoms occur.
Warnings and Precautions
Thrombotic Microangiopathy (TMA) and Thromboembolism Associated With HEMLIBRA and
aPCC
In clinical
trials,
TMA was reported in 0.8% of patients (3/391) and thrombotic events were reported in 0.5% of patients
(2/391).
In patients who received at least one dose of aPCC, TMA was reported in 8.1% of patients (3/37) and
thrombotic events were reported in 5.4% of patients (2/37).
Patients with TMA presented with thrombocytopenia, microangiopathic hemolytic anemia, and acute
kidney
injury, without severe deficiencies in ADAMTS13.
Consider the benefits and risks if aPCC must be used in a patient receiving HEMLIBRA prophylaxis. Due to the long half-life of HEMLIBRA, the potential for an interaction with aPCC may persist for up to 6 months after the last dose. Monitor for the development of TMA and/or thromboembolism when administering aPCC. Immediately discontinue aPCC and interrupt HEMLIBRA prophylaxis if clinical symptoms, imaging, or laboratory findings consistent with TMA and/or thromboembolism occur, and manage as clinically indicated. Consider the benefits and risks of resuming HEMLIBRA prophylaxis following complete resolution of TMA and/or thrombotic events on a case-by-case basis.
Immunogenicity
Treatment with HEMLIBRA may induce anti-drug antibodies. Anti-emicizumab-kxwh antibodies were reported in 5.1% of patients (34/668) treated with HEMLIBRA in clinical trials. Most patients with anti-emicizumab-kxwh antibodies did not experience a change in HEMLIBRA plasma concentrations or an increase in bleeding events; however, in uncommon cases (incidence <1%), the presence of neutralizing antibodies with decreasing plasma concentration may be associated with loss of efficacy.
Monitor for clinical signs of loss of efficacy (eg, increase in breakthrough bleeding events) and if observed, promptly assess the etiology and consider a change in treatment if neutralizing anti-emicizumab-kxwh antibodies are suspected.
Laboratory Coagulation Test Interference
HEMLIBRA affects intrinsic pathway clotting-based laboratory tests, including activated clotting time (ACT); activated partial thromboplastin time (aPTT); and all assays based on aPTT, such as one-stage, factor VIII (FVIII) activity. Therefore, intrinsic pathway clotting-based coagulation laboratory test results in patients who have been treated with HEMLIBRA prophylaxis should not be used to monitor HEMLIBRA activity, determine dosing for factor replacement or anti-coagulation, or measure FVIII inhibitor titers.
Results affected by HEMLIBRA: aPTT; Bethesda assays (clotting-based) for FVIII inhibitor titers; one-stage, aPTT-based single-factor assays; aPTT-based Activated Protein C Resistance (APC-R); ACT.
Results unaffected by HEMLIBRA: Bethesda assays (bovine chromogenic) for FVIII inhibitor titers; thrombin time (TT); one-stage, prothrombin time (PT)-based single-factor assays; chromogenic-based single-factor assays other than FVIII (see Drug Interactions for FVIII chromogenic activity assay considerations); immuno-based assays (ie, ELISA, turbidimetric methods); genetic tests of coagulation factors (eg, Factor V Leiden, Prothrombin 20210).
Most Common Adverse Reactions
The most common adverse reactions (incidence ≥10%) are injection site reactions, headache, and arthralgia.
Adverse Reactions
Characterization of aPCC Treatment in Pooled Clinical Trials
There were 130 instances of aPCC treatment in 37 patients, of which 13 instances (10%) consisted of on average a cumulative amount of >100 U/kg/24 hours of aPCC for 24 hours or more; 2 of the 13 were associated with thrombotic events and 3 of the 13 were associated with TMA. No TMA or thrombotic events were associated with the remaining instances of aPCC treatment.
Injection Site Reactions
In total, 85 patients (22%) reported injection site reactions (ISRs). All ISRs observed in HEMLIBRA clinical trials were reported as mild to moderate intensity and 93% resolved without treatment. The commonly reported ISR symptoms were injection site erythema (11%), injection site pruritus (4%), and injection site pain (4%).
Other Less Common (<1%) Reactions
Rhabdomyolysis was reported in 2 adult patients with asymptomatic elevations in serum creatine kinase without associated renal or musculoskeletal symptoms. In both instances, the event occurred following an increase in physical activity.
Drug Interactions
Clinical experience suggests that a drug interaction exists with HEMLIBRA and aPCC.
Pregnancy, Lactation, Females and Males of Reproductive Potential
Women of childbearing potential should use contraception while receiving HEMLIBRA. It is not known whether HEMLIBRA can cause fetal harm when administered to a pregnant woman or can affect reproduction capacity. HEMLIBRA should be used during pregnancy only if the potential benefit for the mother outweighs the risk to the fetus. The developmental and health benefits of breastfeeding should be considered along with the mother’s clinical need for HEMLIBRA and any potential adverse effects on the breastfed child from HEMLIBRA or from the underlying maternal condition.
You may report side effects to the FDA at (800) FDA-1088 or www.fda.gov/medwatch. You may also report side effects to Genentech at (888) 835-2555.
Please see the HEMLIBRA full Prescribing Information for additional Important Safety Information, including Boxed WARNING.
AE=adverse event; aPCC=activated prothrombin complex concentrate; ASP=average sales price; CI=confidence interval; EHL=extended half-life; Embase=Excerpta Medica Database; ER=emergency room; HCRU=healthcare resource utilization; IQR=interquartile range; ISR=injection site reaction; PwHA=people with hemophilia A; QW=every week; Q2W=every 2 weeks; Q4W=every 4 weeks; SHL=standard half-life; TE=thrombotic event; TMA=thrombotic microangiopathy; WAC=wholesale acquisition cost.
References
- 1. Data on file. Genentech, Inc.
- 2. Genentech. FDA approves Genentech’s Hemlibra (emicizumab-kxwh) for hemophilia A without factor VIII inhibitors. Accessed June 26, 2025. https://www.gene.com/media/press-releases/14749/2018-10-04/fda-approves-genentechs-hemlibra-emicizu.
- 3. US Food and Drug Administration. FDA approves emicizumab-kxwh for prevention and reduction of bleeding in patients with hemophilia A with factor VIII inhibitors. Accessed June 26, 2025. https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-emicizumab-kxwh-prevention-and-reduction-bleeding-patients-hemophilia-factor-viii
- 4. US Food and Drug Administration. FDA approves emicizumab-kxwh for hemophilia A with or without factor VIII inhibitors. Accessed June 26, 2025. https://www.fda.gov/drugs/drug-approvals-and-databases/fda-approves-emicizumab-kxwh-hemophilia-or-without-factor-viii-inhibitors
- 5. HEMLIBRA [package insert]. South San Francisco, CA: Genentech, Inc.; 2025.
- 6. National Bleeding Disorders Foundation. MASAC document #268. Recommendation on the use and management of emicizumab-kxwh (Hemlibra®) for hemophilia A with and without Inhibitors. Accessed June 26, 2025. https://www.bleeding.org/sites/default/files/document/files/268_Emicizumab.pdf
- 7. Young G, Liesner R, Chang T, et al. A multicenter, open-label phase 3 study of emicizumab
prophylaxis in children with hemophilia A with inhibitors. Blood.
2019;134(24):2127-2138. doi:10.1182/blood.2019001869 - 8. Hoffmann-La Roche. Efficacy, safety, and pharmacokinetic study of prophylactic emicizumab versus no prophylaxis in hemophilia A participants (HAVEN 5). Accessed June 26, 2025. https://clinicaltrials.gov/study/NCT03315455?term=emicizumab&rank=10
- 9. Shima M, Nogami K, Nagami S, et al. A multicentre, open-label study of emicizumab given every 2 or 4 weeks in children with severe haemophilia A without inhibitors. Haemophilia. 2019;25(6):979-987. doi:10.1111/hae.13848
- 10. Jiménez-Yuste V, Peyvandi F, Klamroth R, et al. Safety and efficacy of long-term emicizumab prophylaxis in hemophilia A with factor VIII inhibitors: A phase 3b, multicenter, single-arm study (STASEY). Res Pract Thromb Haemost. 2022;6(8):e12837. doi:10.1002/rth2.12837
- 11. Négrier C, Mahlangu J, Lehle M, et al. Emicizumab in people with moderate or mild haemophilia A (HAVEN 6): a multicentre, open-label, single-arm, phase 3 study. Lancet Haematol. 2023;10(3):e168-e177. doi:10.1016/S2352-3026(22)00377-5
- 12. Pipe SW, Collins P, Dhalluin C, et al. Emicizumab prophylaxis in infants with hemophilia A (HAVEN
7): primary analysis of a phase 3b open-label trial. Blood.
2024;143(14):1355-1364. doi:10.1182/blood.2023021832 - 13. Lee JS, To TM, Schuldt R, Lee L, Ahuja S. Impact of emicizumab on real-world healthcare resource utilization in the US. Poster presented at: Academy of Managed Care Pharmacy Nexus 2025; October 27-30, 2025; National Harbor, MD. Poster 232.
- 14. Curtis R, Decker-Palmer M, Wilson MR, et al. Cost-effectiveness of emicizumab vs efanesoctocog alfa, standard half life (SHL) and other extended half life (EHL) FVIII products for prophylaxis in people with severe hemophilia a without inhibitors. Poster presented at: Annual Meeting of the American Society of Hematology; December 9-12, 2023; San Diego, CA.
- 15. Shapiro AD, Schuldt R, Xia Z, et al. Real-world adherence and persistence to emicizumab using a
national US claims database. Poster presented at: the 66th ASH Annual
Meeting; December 7-10, 2024; San Diego CA. - 16. Recht M, et al. Real-world experience with emicizumab for hemophilia a from the physician
perspective based on survey data. Blood. 2024;144(supp 1):5078–5079. doi:10.1182/
blood-2024-200784 - 17. National Bleeding Disorders Foundation. MASAC document #267. MASAC recommendation concerning
prophylaxis for hemophilia A and B with and without inhibitors. Accessed June 26, 2025. https://www.bleeding.org/sites/default/files/document/files/
267_Prophylaxis.pdf - 18. Callaghan MU, Negrier C, Paz-Priel I, et al. Long-term outcomes with emicizumab prophylaxis for hemophilia A with or without FVIII inhibitors from the HAVEN 1-4 studies. Blood. 2021;137(16):2231-2242. doi:10.1182/blood.2020009217
Intended for distribution only to payers, formulary committees, or similar entities for healthcare economic analysis to facilitate drug selection, on a population basis, for coverage or reimbursement.

HEMLIBRA® is a registered trademark of Chugai Pharmaceutical Co., Ltd., Tokyo, Japan.
The HEMLIBRA logo is a registered trademark of Chugai Pharmaceutical Co., Ltd., Tokyo, Japan.
The Genentech logo is a registered trademark of Genentech, Inc.
All other trademarks are the property of their respective owners.
© 2026 Genentech USA, Inc. All rights reserved. M-US-00029193(v1.0) 11/25
