





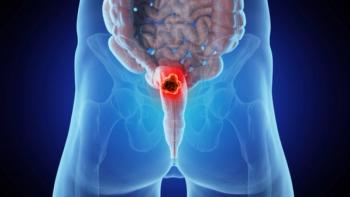
Patients with colorectal liver metastases had local tumor progression when they had minimal ablative margin from intraprocedural contrast-enhanced computed tomography.
Patients with colorectal liver metastases had local tumor progression when they had minimal ablative margin from intraprocedural contrast-enhanced computed tomography.

Tumor location, tumor size, and T stage associated with patients with rectal cancer who have inferior mesenteric artery lymph node metastases.

The Shield blood test developed by Guardant has been approved by the FDA as a primary screening option for colorectal cancer, providing a more convenient method of screening.

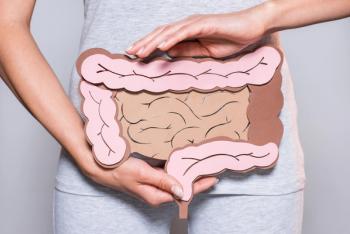
Patients diagnoesd with metabolic dysfunction–associated steatotic liver disease may have a higher risk of colorectal cancer (CRC) or colorectal adenoma.

Overall and site-specific colorectal cancer (CRC) had a negative association with the usage of aspirin.

A nomogram model that included log odd of positive lymph node was effective in predicting prognosis of early-onset colorectal cancer (EOCRC).

Between 2016 and 2021, the percentage of screening colonoscopies performed by a family physician saw a decrease across the country.

In a recent study, novel genetic associations between obesity, colorectal cancer (CRC), and irritable bowel disease (IBD) were identified.
Patients who used adjuvant chemotherapy were found to have a higher survival rate after achieving complete pathological response.
Adult patients who have KRAS G12C-mutated locally advanced or metastatic colorectal cancer (CRC) can use adagrasib as a supplemental treatment.

Both preoperative pan-immune inflammation value (PIV) and monocyte to high-density lipoprotein ratio (MHR) were found to be independent risk factors when it came to the prognosis for colorectal cancer (CRC).

Older adults who had colorectal surgery were found to have reduced postoperative complications if they started the Geriatric Oncology Service.

A recent review found that benzene exposure due to work may be linked to the development of colorectal cancer.

A dose escalation strategy for regorafenib could improve the cost-effectiveness of the medication in metastatic colorectal cancer (CRC).

The Hospital Frailty Risk Score, Secondary Care Administrative Records Frailty index, and the frailty syndromes measures were able to assess frailty in patients diagnosed with colorectal cancer (CRC).

Clinical use of liquid biopsies to determine the likelihood of CRC is the goal based on its effectiveness in recent studies.
MicroRNAs could be a key to future testing for colorectal cancer (CRC) and determining treatment.
Ajay Goel, PhD, AGAF, discusses study findings that could help in earlier detection of lymph node metastases and colorectal cancer (CRC).
The CDC has asked local and state health officials to maintain peak-season flu surveillance operation levels over the summer to watch for any signs of human-to-human spread of the H5N1 bird flu virus; the drug industry’s top lobbying group faced thorough questioning at a Senate Judiciary Committee hearing about the impact of patent system abuse on high prescription drug prices; FDA staff reviewers have raised concerns that Guardant Health’s colorectal cancer (CRC) blood test may fail to detect precancerous tumors.
Ajay Goel, PhD, AGAF, explains the significance of 2 new studies that found that early-onset colorectal cancer (EOCRC) and recurrence in CRC could both be predicted using new blood and tissue tests.
Patients with colorectal cancer (CRC) had lower 5-year survival if they had type 2 diabetes.

Robot-assisted laparoscopic surgery was found to be more effective in harvesting lymph nodes compared with conventional surgery with similar outcomes.
Restoring diurnal rest-activity rhythm in patients who have had surgery for colorectal cancer (CRC) can help to improve their sleep patterns and quality of life (QOL).
A study found significant incidence of advanced neoplasia in patients who had a colonoscopy to screen for colorectal cancer (CRC) when aged more than 75 years.

Blood-based screening for colorectal cancer (CRC) should only be used with patients who are not completing other endorsed screening options, according to a study.